Waiver Of Health Coverage Form
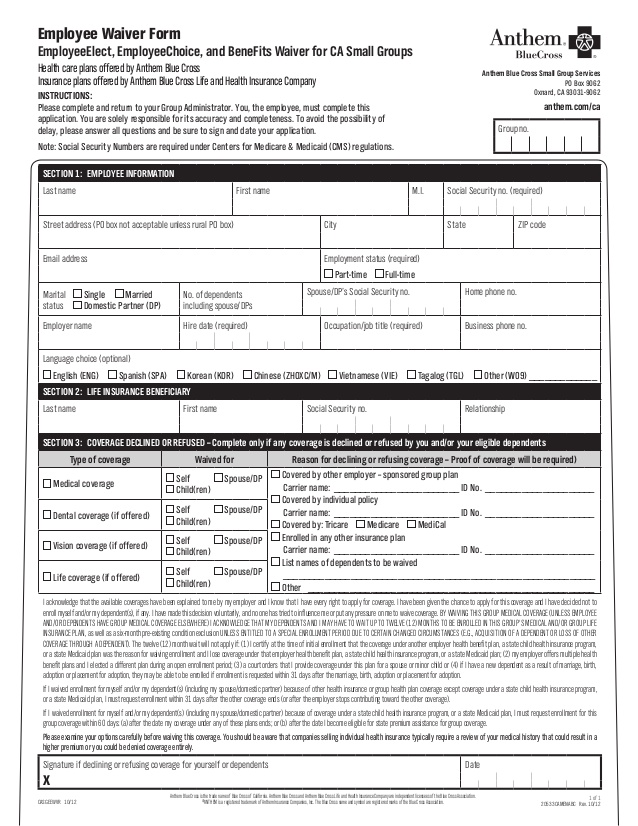
Waiver Of Health Coverage Form - Attach a photocopy of the plan provider id card. If your employer offers multiple choices of health insurance plans, please complete the following section: If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. I am waiving bcn coverage from my. Read the statement carefully, then sign and date the waiver of coverage form. This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the.
If your employer offers multiple choices of health insurance plans, please complete the following section: I am waiving bcn coverage from my. This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. Read the statement carefully, then sign and date the waiver of coverage form. Attach a photocopy of the plan provider id card.
If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. Attach a photocopy of the plan provider id card. If your employer offers multiple choices of health insurance plans, please complete the following section: I am waiving bcn coverage from my. Read the statement carefully, then sign and date the waiver of coverage form.
FREE 9+ Health Waiver Forms in PDF Ms Word
I am waiving bcn coverage from my. If your employer offers multiple choices of health insurance plans, please complete the following section: This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. Read the statement carefully, then sign and date the waiver of coverage form. If you declined.
FREE 13+ Health Insurance Form Samples, PDF, MS Word, Google Docs
This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. I am waiving bcn coverage from my. If your employer offers multiple choices of health insurance plans, please complete the following section: If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be.

Waiver Template Word
If your employer offers multiple choices of health insurance plans, please complete the following section: Attach a photocopy of the plan provider id card. I am waiving bcn coverage from my. If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. Read the statement carefully, then sign and date.
FREE 9+ Health Waiver Forms in PDF Ms Word
I am waiving bcn coverage from my. If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. Read the statement carefully, then sign and date the waiver of coverage form. Attach a photocopy of the plan provider id card. This waiver form must be completed by any eligible employee.
Kaiser Group Health Insurance Waiver
Read the statement carefully, then sign and date the waiver of coverage form. I am waiving bcn coverage from my. If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. If your employer offers multiple choices of health insurance plans, please complete the following section: Attach a photocopy of.
FREE 9+ Sample Medical Waiver Forms in PDF MS Word
Read the statement carefully, then sign and date the waiver of coverage form. If your employer offers multiple choices of health insurance plans, please complete the following section: Attach a photocopy of the plan provider id card. If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. I am.

Benefits Waiver Form Fill Online, Printable, Fillable, Blank pdfFiller
If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. Read the statement carefully, then sign and date the waiver of coverage form. This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. If your employer offers.
Health Insurance Waiver Form Template amulette
If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. Read the statement carefully, then sign and date the waiver of coverage form. If your employer offers multiple choices of health insurance plans, please complete the following section: I am waiving bcn coverage from my. Attach a photocopy of.
FREE 10+ Medical Waiver Forms in PDF MS Word
Read the statement carefully, then sign and date the waiver of coverage form. If your employer offers multiple choices of health insurance plans, please complete the following section: This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. Attach a photocopy of the plan provider id card. If.
Printable Insurance Waiver Form Printable Forms Free Online
If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or. Read the statement carefully, then sign and date the waiver of coverage form. Attach a photocopy of the plan provider id card. If your employer offers multiple choices of health insurance plans, please complete the following section: I am.
I Am Waiving Bcn Coverage From My.
Attach a photocopy of the plan provider id card. If your employer offers multiple choices of health insurance plans, please complete the following section: This waiver form must be completed by any eligible employee who has voluntarily elected to waive his/her opportunity to participate in the. If you declined enrollment for yourself or your dependent(s) (including a spouse/domestic partner), you may be able to enroll yourself or.