Vsp Claim Form Pdf
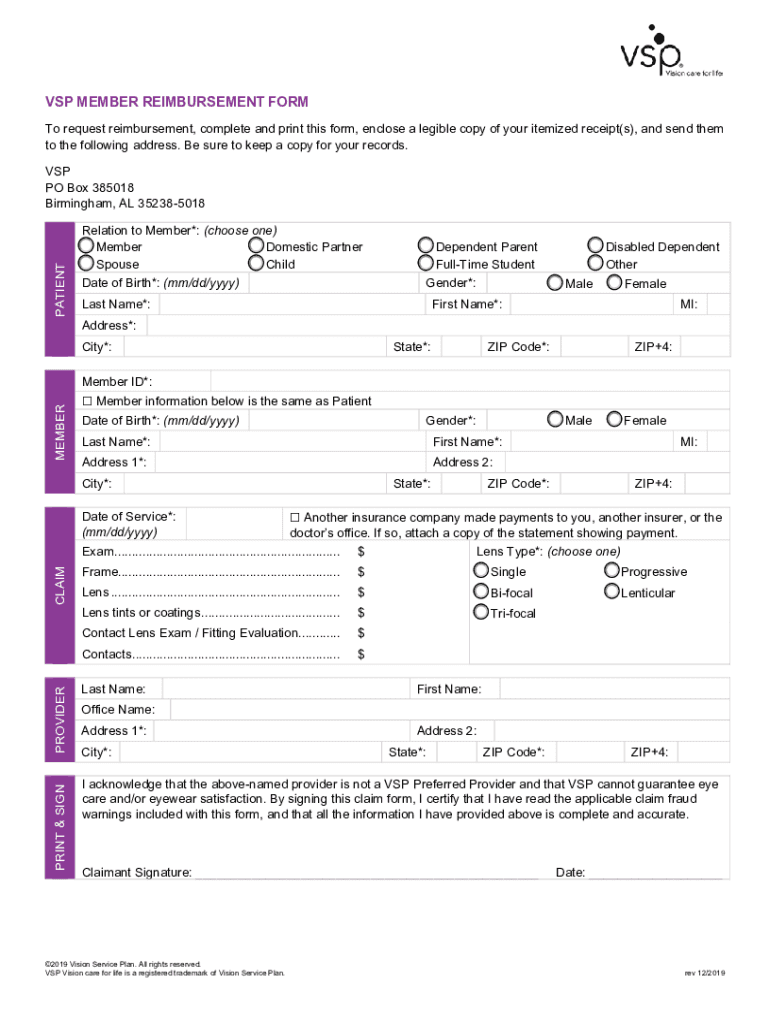
Vsp Claim Form Pdf - Submit this form along with your **itemized receipt to: 1a enter insured’s id number. Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. 1 check the box(es) that identifies the type of health insurance coverage(s) applicable.
Submit this form along with your **itemized receipt to: To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. 1 check the box(es) that identifies the type of health insurance coverage(s) applicable. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. 1a enter insured’s id number.
1 check the box(es) that identifies the type of health insurance coverage(s) applicable. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. Submit this form along with your **itemized receipt to: 1a enter insured’s id number.
Fillable Online Vision Service Plan (VSP) reimbursement form Fax Email
Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. 1a enter insured’s id number. 1 check the box(es) that identifies the type of health insurance coverage(s) applicable. Submit this form along with your **itemized receipt to: Fill out the form completely and if you're filling it out online,.
Form University Fill Online, Printable, Fillable
Submit this form along with your **itemized receipt to: To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. 1a enter insured’s id number. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim.

Vsp Claim Form Printable Printable Word Searches
1 check the box(es) that identifies the type of health insurance coverage(s) applicable. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to.
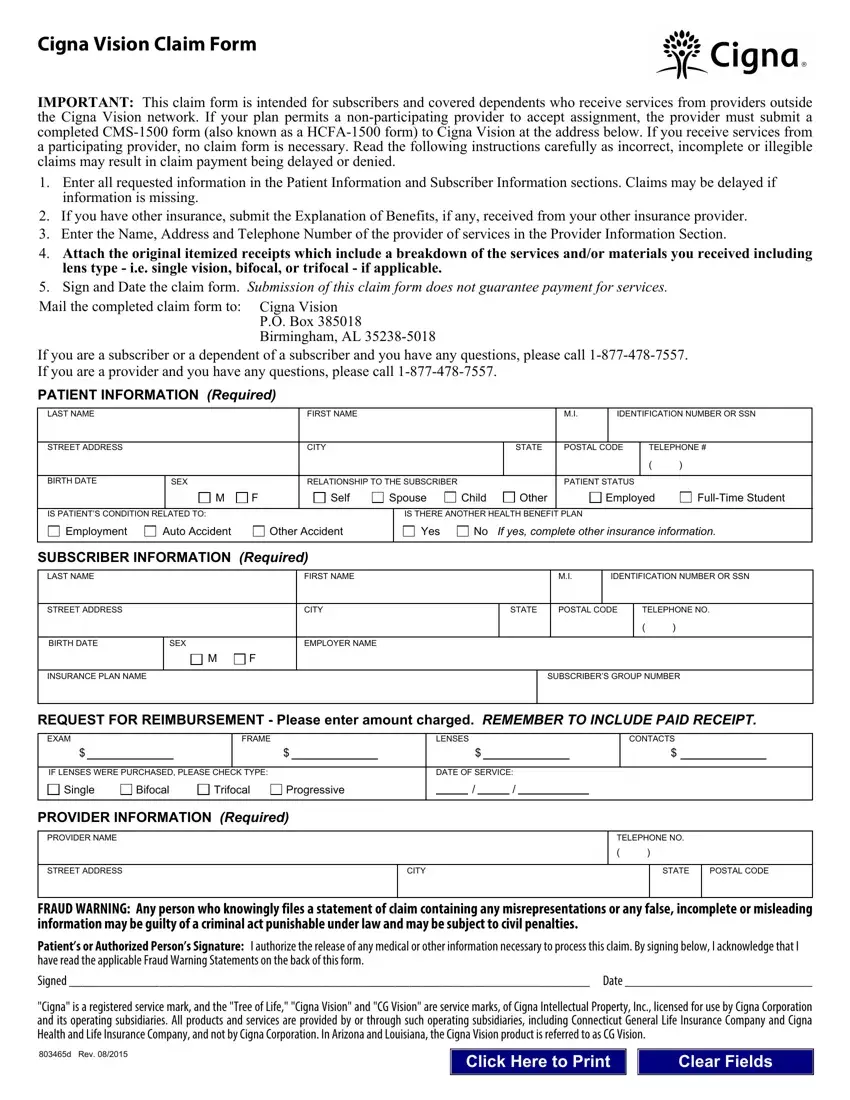
Cigna Vision Claim Form ≡ Fill Out Printable PDF Forms Online
To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. 1 check the box(es) that identifies the type of health insurance coverage(s) applicable. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to.

Vsp Vision Claim Form
Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. Submit this form along with your **itemized receipt to: 1a enter insured’s id number. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. Fill out the.
Vsp Printable Claim Form Printable Forms Free Online
1 check the box(es) that identifies the type of health insurance coverage(s) applicable. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. Submit this form along with your **itemized receipt to: 1a enter insured’s id number. To request reimbursement, complete and print.

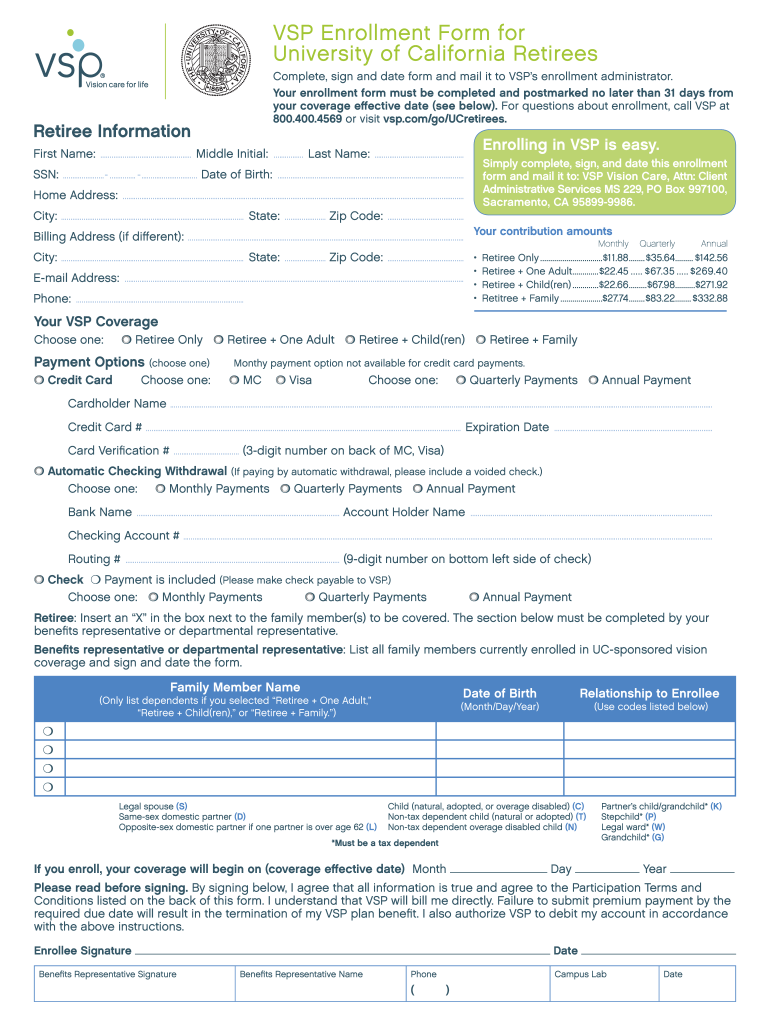
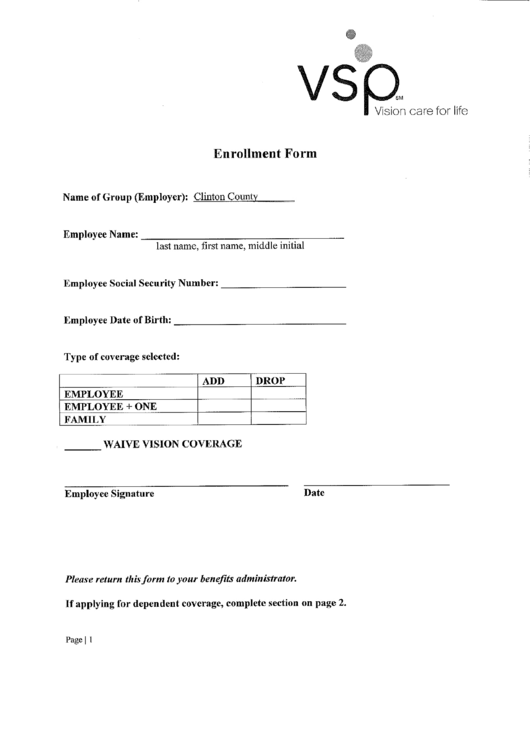
Vsp Enrollment Form Fill Online, Printable, Fillable, Blank pdfFiller
Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. 1a enter insured’s id number. Submit this form along with your **itemized receipt to: Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to.

Vsp Enrollment Form 2020 Pdf Fill Online Printable Fillable Blank
Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. 1 check the box(es) that identifies the type of health insurance coverage(s) applicable. 1a enter insured’s id number. To request reimbursement, complete and print this form, enclose a legible copy of your itemized.

Vsp Claim Form Printable Printable Word Searches
1a enter insured’s id number. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. Submit this form along with your **itemized.

Vsp reimbursement form pdf Fill out & sign online DocHub
Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. Fill out the form completely and if you're filling it out online, snap a picture of your receipt and attach it to your claim to get your. 1a enter insured’s id number. 1 check the box(es) that identifies the.
Fill Out The Form Completely And If You're Filling It Out Online, Snap A Picture Of Your Receipt And Attach It To Your Claim To Get Your.
Vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your. 1 check the box(es) that identifies the type of health insurance coverage(s) applicable. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following. Submit this form along with your **itemized receipt to: