Refusal Of Treatment Form
Refusal Of Treatment Form - By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I have had an opportunity to. I am provided with this refusal form and information so i may understand the recommended treatment and the consequences of refusing treatment. (see our sample form “refusal to consent to treatment, medication, or testing.”) although a form is optional, it offers practitioners the strongest protection against subsequent claims. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider.
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I am provided with this refusal form and information so i may understand the recommended treatment and the consequences of refusing treatment. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: (see our sample form “refusal to consent to treatment, medication, or testing.”) although a form is optional, it offers practitioners the strongest protection against subsequent claims. I have had an opportunity to.
I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I am provided with this refusal form and information so i may understand the recommended treatment and the consequences of refusing treatment. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. I have had an opportunity to. (see our sample form “refusal to consent to treatment, medication, or testing.”) although a form is optional, it offers practitioners the strongest protection against subsequent claims.
Refusal Of Dental Treatment Form printable pdf download
I am provided with this refusal form and information so i may understand the recommended treatment and the consequences of refusing treatment. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. (see our sample form “refusal to consent to treatment, medication, or testing.”).
√ 20 Refusal Of Treatment form Sample ™ Dannybarrantes Template
I have had an opportunity to. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: I am provided with this refusal form and information so.
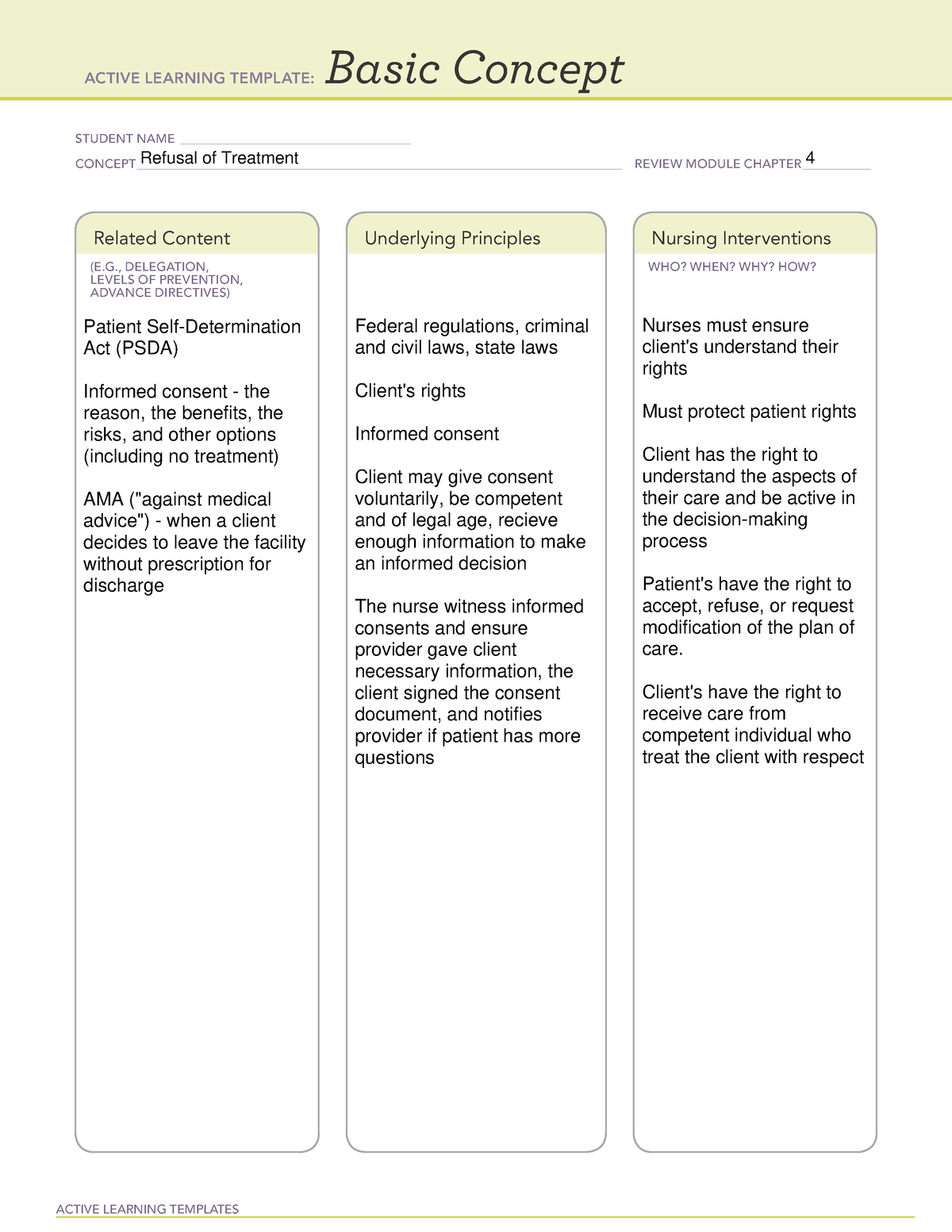
ATI template refusal of treatment ACTIVE LEARNING TEMPLATES Basic
(see our sample form “refusal to consent to treatment, medication, or testing.”) although a form is optional, it offers practitioners the strongest protection against subsequent claims. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I am provided with this refusal form.

Refusal of Dental Treatment Form PDF airSlate SignNow
This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: I have had an opportunity to. By signing below, i understand that my refusal to follow.
Refusal of Medical Treatment or Observation
I have had an opportunity to. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: I am provided with this refusal form and information.
Against medical advice form Fill out & sign online DocHub
I have had an opportunity to. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: I am provided with this refusal form and information so i may understand the recommended treatment and the consequences of refusing treatment. By signing below, i understand that my refusal to follow my providers advice and.

Medical Treatment Refusal Form Template amulette
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. (see our sample form “refusal to consent to treatment, medication, or testing.”) although a form is optional, it offers practitioners the strongest protection against subsequent claims. I, _____, refuse to consent to the.
Top 10 Refusal Of Medical Treatment Form Templates free to download in
This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I, _____, refuse to consent to the.
Top 10 Refusal Of Medical Treatment Form Templates free to download in
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by his/her physician or provider. I have had an opportunity to. (see.

Refusal Of Medical Treatment Form California 20202022 Fill and Sign
I am provided with this refusal form and information so i may understand the recommended treatment and the consequences of refusing treatment. I have had an opportunity to. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: By signing below, i understand that my refusal to follow my providers advice and.
I Am Provided With This Refusal Form And Information So I May Understand The Recommended Treatment And The Consequences Of Refusing Treatment.
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I have had an opportunity to. (see our sample form “refusal to consent to treatment, medication, or testing.”) although a form is optional, it offers practitioners the strongest protection against subsequent claims. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: