Physical Therapy Screening Form
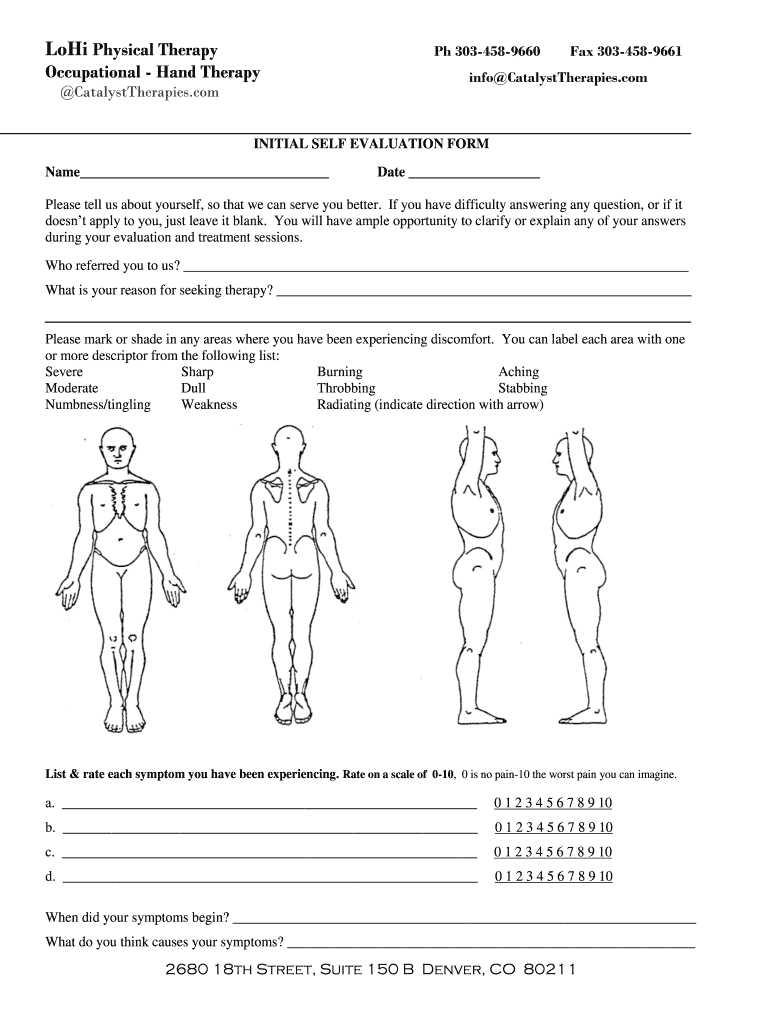
Physical Therapy Screening Form - Date of birth date of injury or symptoms. What brings you to pt today? To ensure a thorough evaluation, please provide this important information about your medical history. Please answer all of the questions in the following survey. Please complete both sides of form. Please circle each condition that you have been told you have (or had). These questions will ask you if you. What is your personal goal for therapy? Patient’s name chief complaints or concern. If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be.
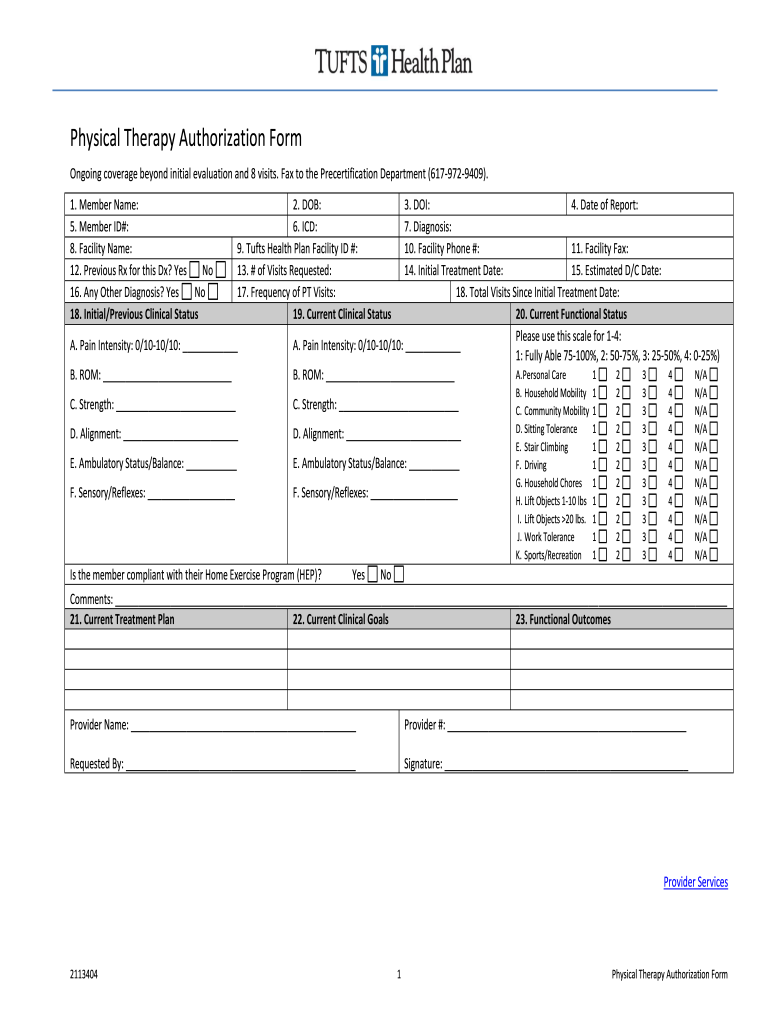
Date of birth date of injury or symptoms. This physical therapy intake form is essential for new patients to provide their personal and health history before initial appointments. What is your personal goal for therapy? Patient’s name chief complaints or concern. What brings you to pt today? These questions will ask you if you. If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be. To ensure a thorough evaluation, please provide this important information about your medical history. Please complete both sides of form. Please answer all of the questions in the following survey.
This physical therapy intake form is essential for new patients to provide their personal and health history before initial appointments. Patient’s name chief complaints or concern. These questions will ask you if you. Please complete both sides of form. To ensure a thorough evaluation, please provide this important information about your medical history. What is your personal goal for therapy? If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be. Please circle each condition that you have been told you have (or had). Please answer all of the questions in the following survey. What brings you to pt today?
19+ Physical Therapy Initial Evaluation Form DocTemplates
Please answer all of the questions in the following survey. Date of birth date of injury or symptoms. Please complete both sides of form. If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be. This physical therapy intake form is essential for new patients to provide their.
19+ Physical Therapy Initial Evaluation Form DocTemplates
Please circle each condition that you have been told you have (or had). Please answer all of the questions in the following survey. Please complete both sides of form. These questions will ask you if you. What brings you to pt today?
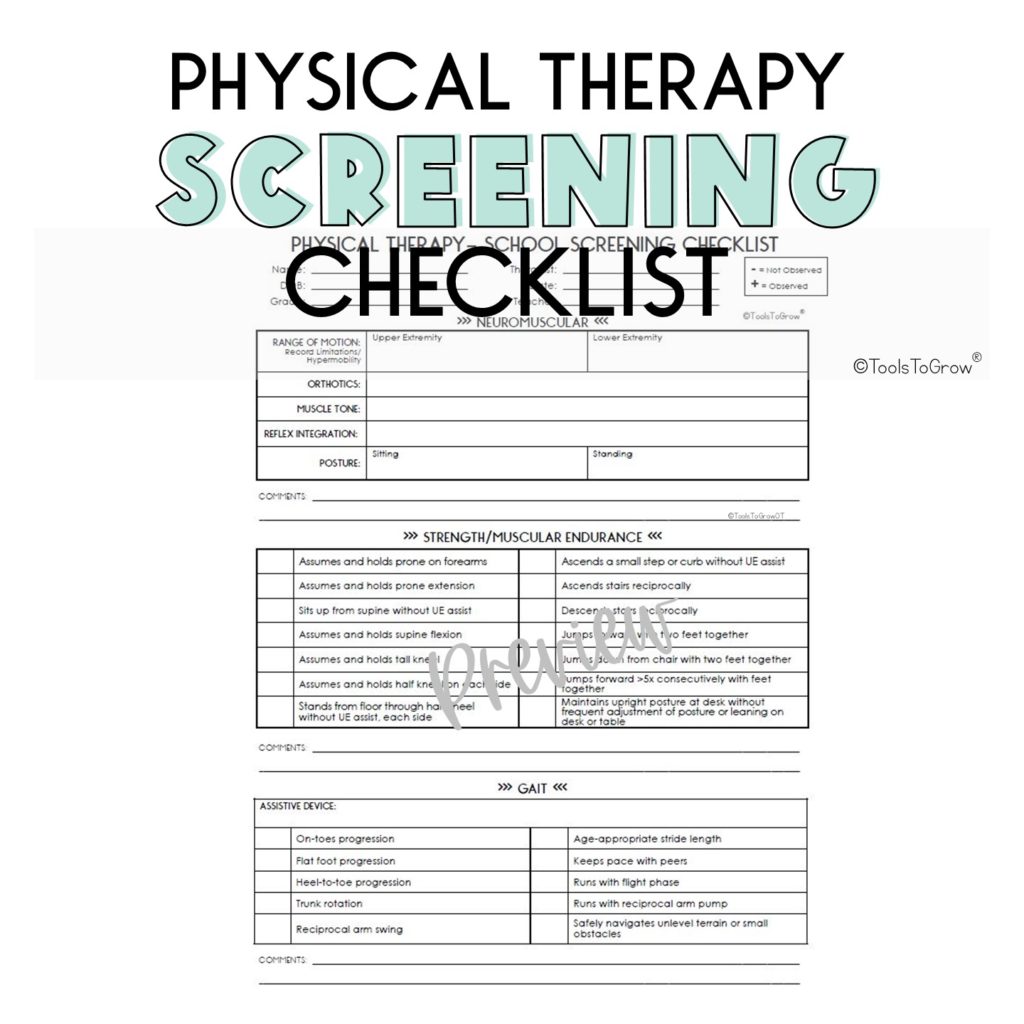
Physical Therapy School Screening Checklist Shop Tools To Grow
Please circle each condition that you have been told you have (or had). If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be. These questions will ask you if you. What is your personal goal for therapy? Please answer all of the questions in the following survey.
Physical Therapy Evaluation 7 Free Download for PDF
These questions will ask you if you. To ensure a thorough evaluation, please provide this important information about your medical history. What is your personal goal for therapy? Please circle each condition that you have been told you have (or had). This physical therapy intake form is essential for new patients to provide their personal and health history before initial.
FREE 15+ Physical Therapy Assessment Form Samples, PDF, MS Word, Google
Please circle each condition that you have been told you have (or had). What brings you to pt today? To ensure a thorough evaluation, please provide this important information about your medical history. What is your personal goal for therapy? Please complete both sides of form.
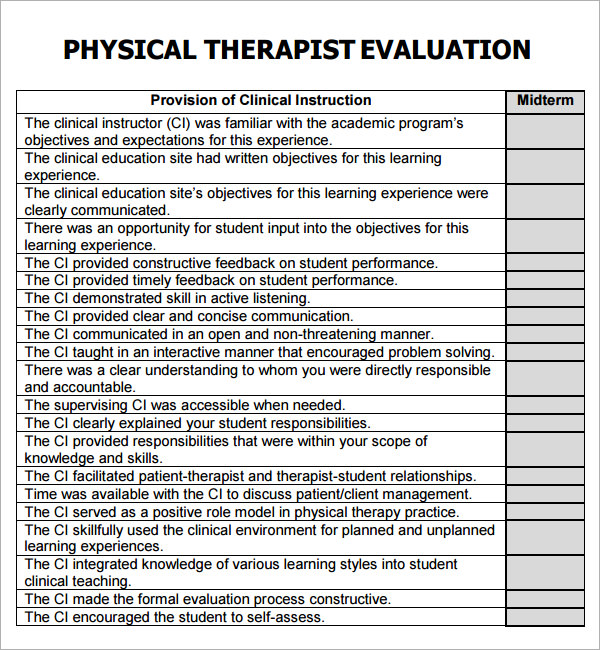
Physical Therapist Evaluation Form Fill Out, Sign Online and Download
To ensure a thorough evaluation, please provide this important information about your medical history. What is your personal goal for therapy? Date of birth date of injury or symptoms. What brings you to pt today? Please circle each condition that you have been told you have (or had).

Physical Therapy Health Screening Form Columbia Memorial
What brings you to pt today? These questions will ask you if you. Please answer all of the questions in the following survey. To ensure a thorough evaluation, please provide this important information about your medical history. If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be.
Section GG SelfCare (Activities of Daily Living) and Mobility Items
What is your personal goal for therapy? Please circle each condition that you have been told you have (or had). What brings you to pt today? Please answer all of the questions in the following survey. This physical therapy intake form is essential for new patients to provide their personal and health history before initial appointments.
Occupational/Physical Therapy Referral Form
What is your personal goal for therapy? What brings you to pt today? These questions will ask you if you. Please answer all of the questions in the following survey. If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be.

Group therapy screening form Fill out & sign online DocHub
These questions will ask you if you. To ensure a thorough evaluation, please provide this important information about your medical history. Patient’s name chief complaints or concern. Date of birth date of injury or symptoms. This physical therapy intake form is essential for new patients to provide their personal and health history before initial appointments.
To Ensure A Thorough Evaluation, Please Provide This Important Information About Your Medical History.
These questions will ask you if you. What brings you to pt today? Patient’s name chief complaints or concern. Please circle each condition that you have been told you have (or had).
What Is Your Personal Goal For Therapy?
Date of birth date of injury or symptoms. This physical therapy intake form is essential for new patients to provide their personal and health history before initial appointments. Please answer all of the questions in the following survey. If you received physical, occupational or speech therapy prior to attending therapy at our center, please be aware that those services will be.