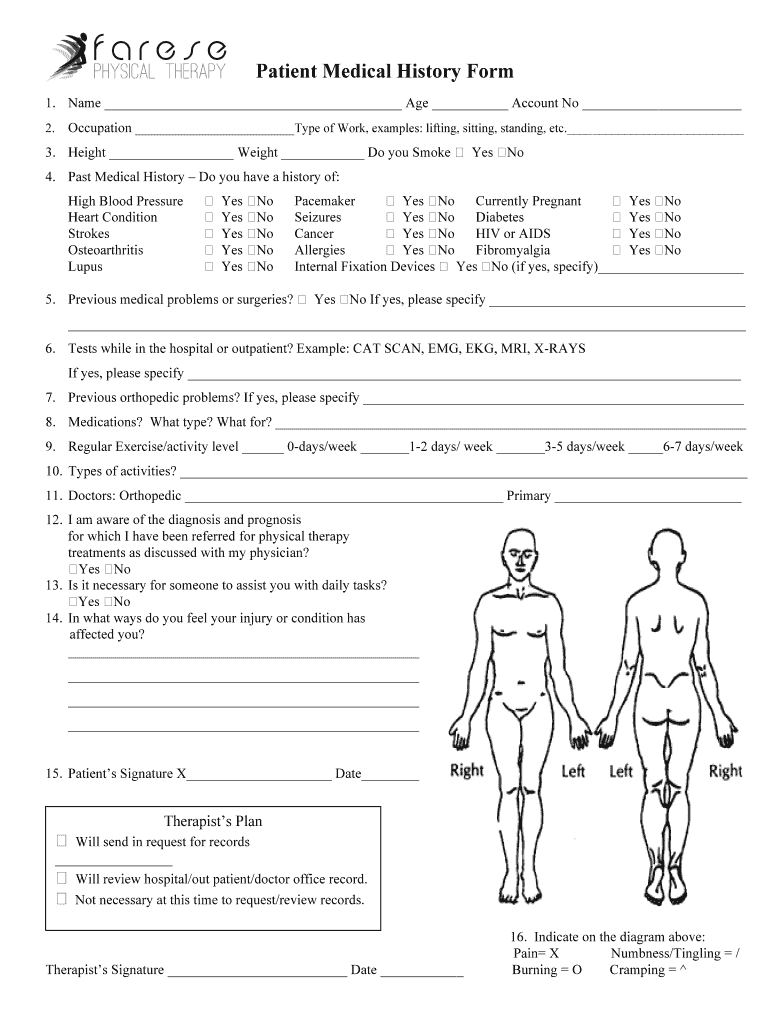
Physical Therapy Medical History Form
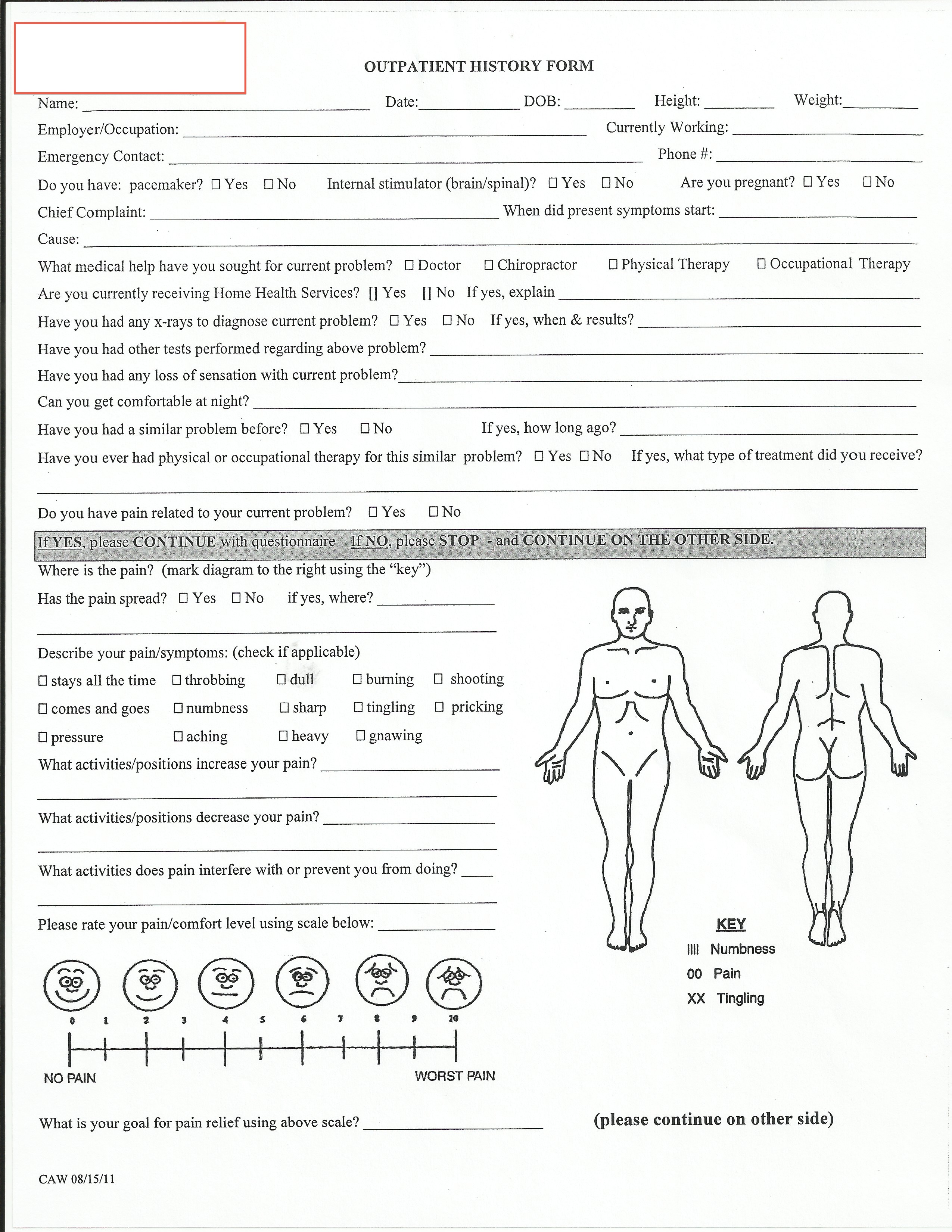
Physical Therapy Medical History Form - The purpose of this questionnaire is to help us perform a thorough evaluation and further understand your. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. The purpose of this questionnaire is to help us understand your health status. List any other prior or current injuries, surgeries, illnesses or medical conditions (including prior episodes of back pain, knee pain, etc.) including. The purpose of this questionnaire is to help the physical therapist understand your health status. Please complete this form and the therapist will. Please complete this form and your therapist will answer any. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. Under medicare and the state practice acts, we are required to obtain a complete medical history on all patients.
List any other prior or current injuries, surgeries, illnesses or medical conditions (including prior episodes of back pain, knee pain, etc.) including. The purpose of this questionnaire is to help us understand your health status. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. The purpose of this questionnaire is to help the physical therapist understand your health status. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. Please complete this form and your therapist will answer any. The purpose of this questionnaire is to help us perform a thorough evaluation and further understand your. Please complete this form and the therapist will. Under medicare and the state practice acts, we are required to obtain a complete medical history on all patients.
List any other prior or current injuries, surgeries, illnesses or medical conditions (including prior episodes of back pain, knee pain, etc.) including. Please complete this form and your therapist will answer any. The purpose of this questionnaire is to help the physical therapist understand your health status. Under medicare and the state practice acts, we are required to obtain a complete medical history on all patients. The purpose of this questionnaire is to help us understand your health status. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. The purpose of this questionnaire is to help us perform a thorough evaluation and further understand your. Please complete this form and the therapist will.
Farese Physical Therapy Patient Medical History Form Fill and Sign
Please complete this form and the therapist will. The purpose of this questionnaire is to help us understand your health status. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the.

Fillable Online Massage Therapy Medical History Form Fax Email Print
The purpose of this questionnaire is to help us understand your health status. The purpose of this questionnaire is to help us perform a thorough evaluation and further understand your. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. The purpose of this questionnaire is to help the physical therapist.

Fillable Online Occupational Hand Therapy Medical History Form Fax
The purpose of this questionnaire is to help the physical therapist understand your health status. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. Please complete this form and the therapist will. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my.
Physical Therapy Evaluation Form
Please complete this form and your therapist will answer any. List any other prior or current injuries, surgeries, illnesses or medical conditions (including prior episodes of back pain, knee pain, etc.) including. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. The purpose of this questionnaire.

Fillable Online med unc UNIVERSITY PHYSICAL THERAPY MEDICAL HISTORY
Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. Please complete this form and your therapist will answer any. The purpose of this questionnaire is to help us understand your health status. Please complete this form and the therapist will. List any other prior or current injuries, surgeries, illnesses or.
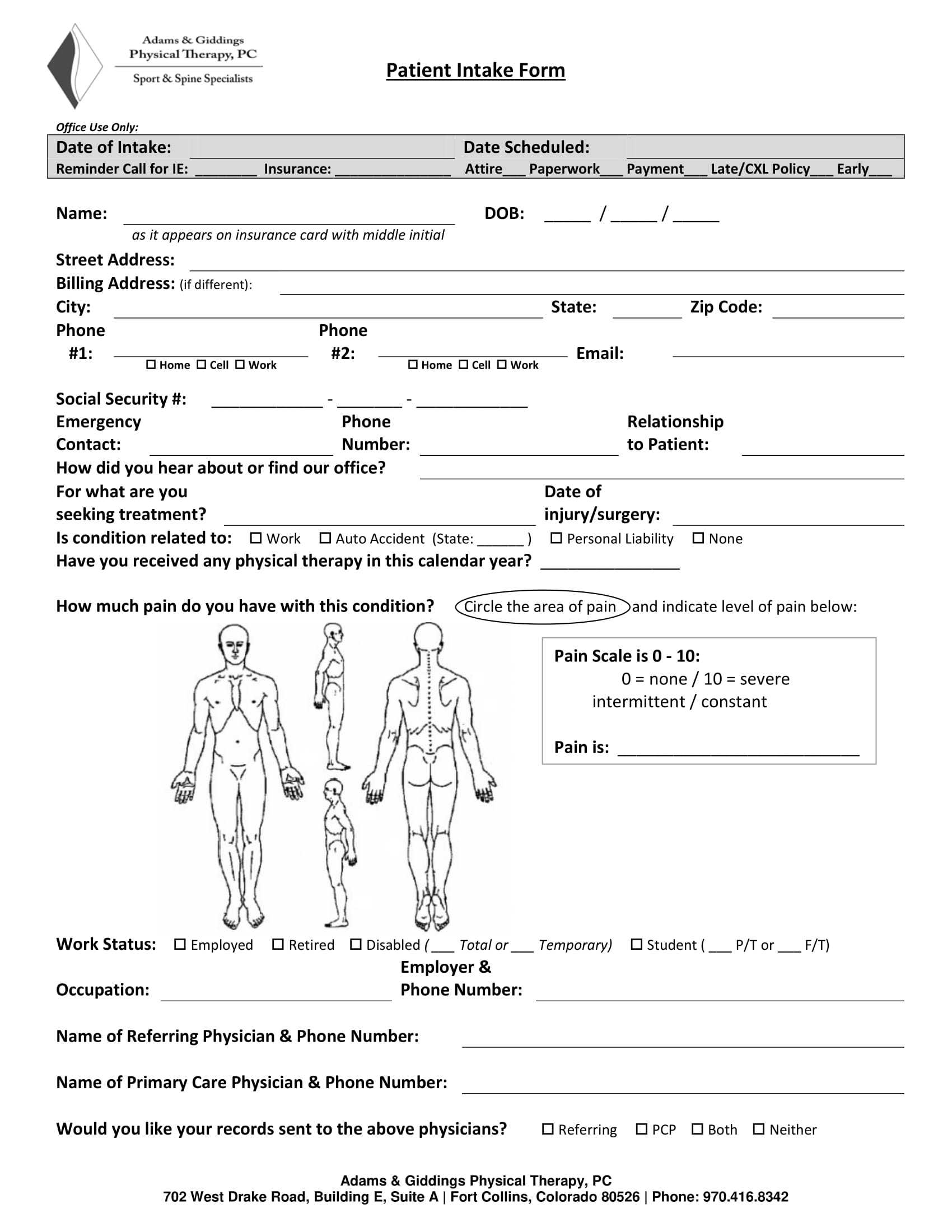
Printable Patient Intake Form
Please complete this form and the therapist will. The purpose of this questionnaire is to help the physical therapist understand your health status. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. Please complete this form and your therapist will answer any. The purpose of this questionnaire is to help.
Free Printable Physical Therapy Evaluation Forms Printable Forms Free
Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. Please complete this form and the therapist will. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. Please complete this form and your therapist will answer any..
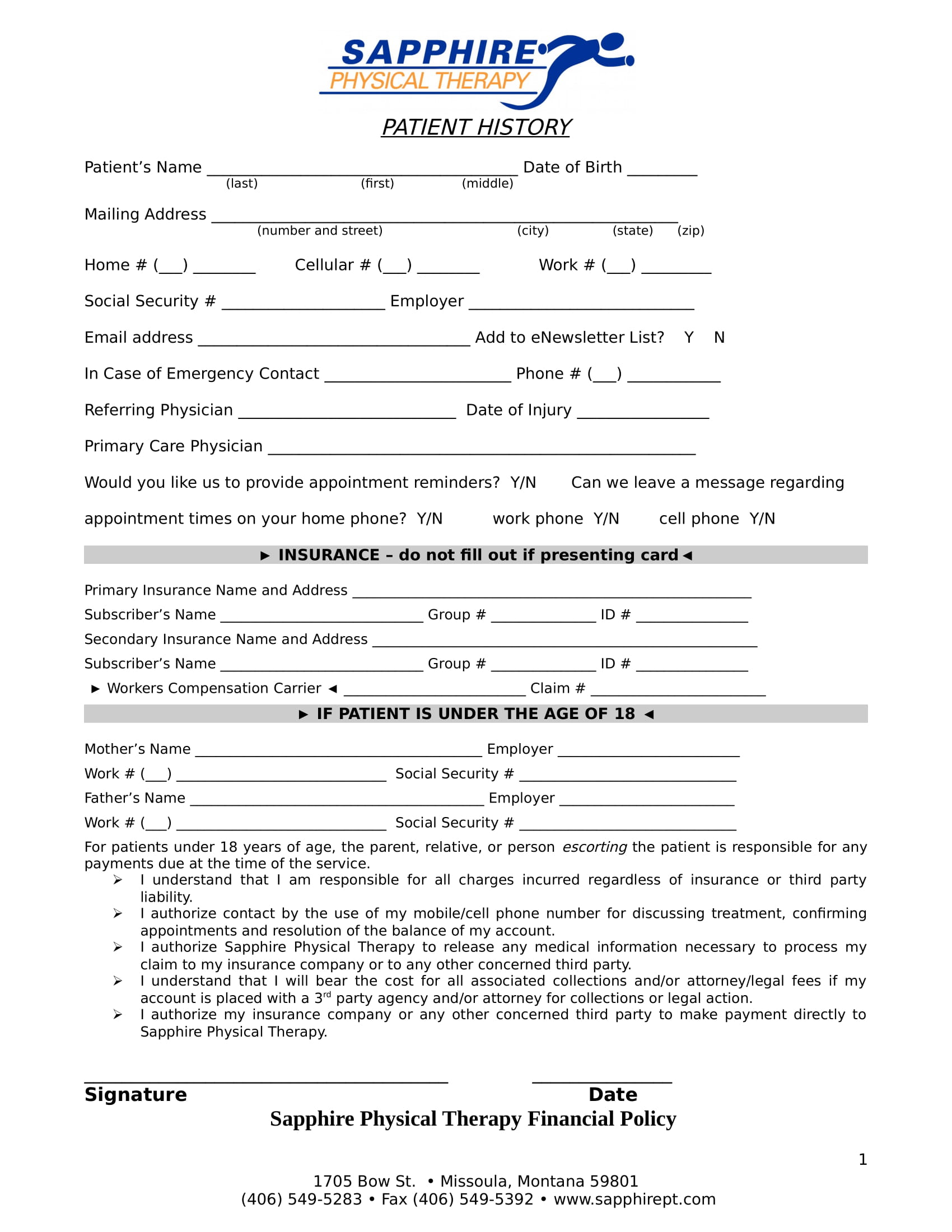
Medical History Form page 1
Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. Please complete this form and your therapist will answer any. Please complete this form and the therapist will. Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important..
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-09-scaled.jpg?w=790)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
The purpose of this questionnaire is to help the physical therapist understand your health status. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. Under medicare and the state practice acts, we are required to obtain a complete medical history on all patients. Please complete this.

Fillable Online LIFE FITNESS PHYSICAL THERAPY MEDICAL HISTORY FORM Fax
List any other prior or current injuries, surgeries, illnesses or medical conditions (including prior episodes of back pain, knee pain, etc.) including. Please complete this form and your therapist will answer any. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. The purpose of this questionnaire.
Please Complete This Form And The Therapist Will.
Physical therapy health history to ensure you receive a complete and thorough evaluation, please provide us with the important. The purpose of this questionnaire is to help the physical therapist understand your health status. The purpose of this questionnaire is to help us perform a thorough evaluation and further understand your. Under medicare and the state practice acts, we are required to obtain a complete medical history on all patients.
The Purpose Of This Questionnaire Is To Help Us Understand Your Health Status.
Please complete this form and your therapist will answer any. Past medical history (please check “yes” if you have ever been diagnosed with.) to the best of my knowledge, the information above is. List any other prior or current injuries, surgeries, illnesses or medical conditions (including prior episodes of back pain, knee pain, etc.) including.