Pap Application Form
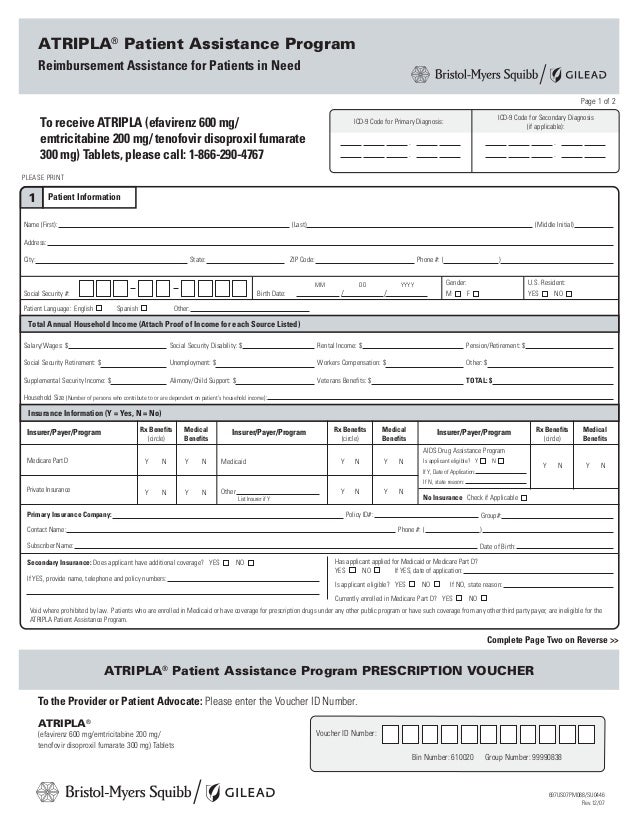
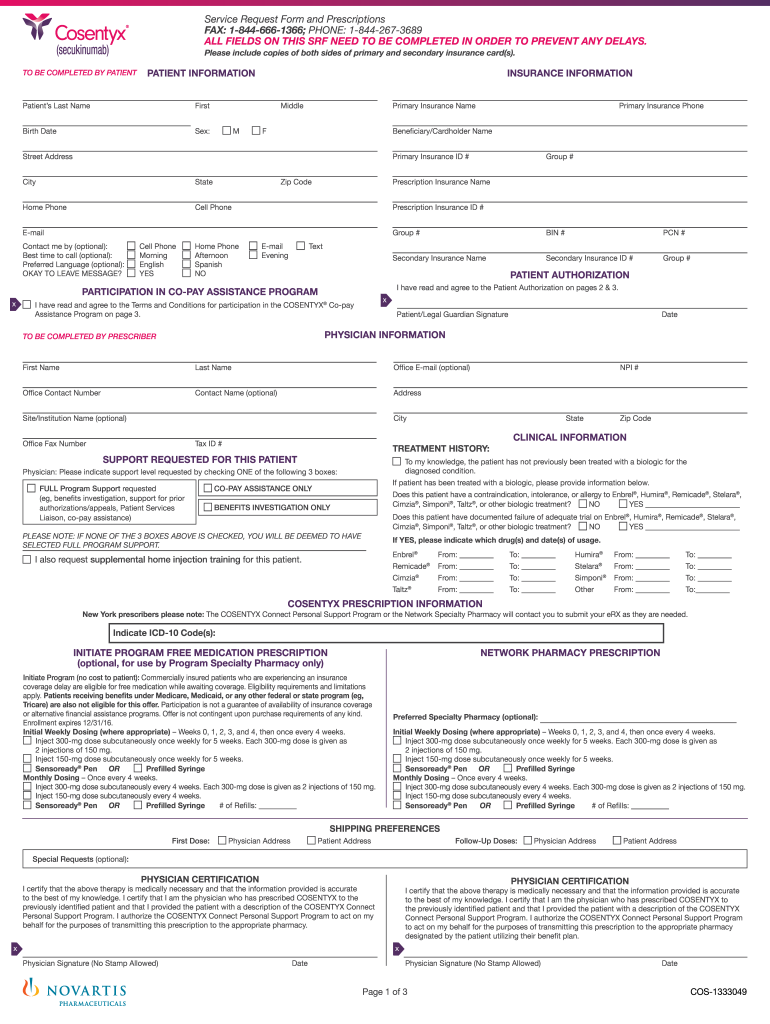
Pap Application Form - Novartis patient assistance foundation, inc. Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to. If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form.
Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. Novartis patient assistance foundation, inc. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the. You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to.
You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the. Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. Novartis patient assistance foundation, inc.

Pap Application 2014 Form Editable 2014 Medicare Part D Medicare
To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. Novartis patient assistance foundation, inc. Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. If the patient is insured and the insurance requires a prior.

PAP Membership Application Form Updated PDF Clinical Psychology
Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and.

Fillable Online es needymeds Enrollment Application for the Novartis
If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the. Novartis patient assistance foundation, inc. Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. To be eligible for pap, both the prescribing.
Pap form
To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. If the patient is insured and the insurance requires a prior authorization (pa), you must submit.

Lillytruassist Application Fill and Sign Printable Template Online
Novartis patient assistance foundation, inc. Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. You authorize abbvie to obtain such information solely to determine patient.
Patient Assistance Program Novartis
If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. Patient assistance connection is part of the program that provides select.

Fillable Online BI Cares PAP Application PDF Fax Email Print pdfFiller
To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to. Novartis patient assistance foundation, inc. If the patient is insured and the insurance requires a prior authorization (pa), you must.

Fillable Online Special PAP application form updated.docx Fax Email
Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to. If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or.

Fillable Online PAP App CR v2 Fax Email Print pdfFiller
Patient assistance connection is part of the program that provides select sanofi prescription medications and vaccines, at no cost, if you. If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the. You authorize abbvie to obtain such information solely to determine patient assistance program.

Fillable Online rxassist OTH11034BMEDA PAP Application Fax Email Print
Novartis patient assistance foundation, inc. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to. If the patient is insured and the insurance requires a prior authorization (pa), you must.
Patient Assistance Connection Is Part Of The Program That Provides Select Sanofi Prescription Medications And Vaccines, At No Cost, If You.
You authorize abbvie to obtain such information solely to determine patient assistance program (pap) eligibility, and to. To be eligible for pap, both the prescribing health care professional and the patient must complete, sign, and date this program application form. Novartis patient assistance foundation, inc. If the patient is insured and the insurance requires a prior authorization (pa), you must submit a copy of the pa and/or appeal outcome for the.