Moda Appeal Form
Moda Appeal Form - Mail this form to moda health: Box 40384, portland, or 97240 or fax to 503. Complaint and appeal form ready to submit? Box 40384, portland, or 97204 or faxed to 503. Medicare appeals unit at p.o. Mail this form to moda health, attn: Submit a written request and mail to: Request for reconsideration should be sent to moda health, attn: Medicare appeal and grievance unit p.o. Mail this form to moda health:
Complaint and appeal form ready to submit? Mail this form to moda health: Box 40384, portland, or 97240 or fax to 503. Box 40384, portland, or 97204 or faxed to 503. Submit a written request and mail to: Medicare appeal and grievance unit p.o. Mail this form to moda health: Request for reconsideration should be sent to moda health, attn: Medicare appeals unit at p.o. Mail this form to moda health, attn:
Box 40384, portland, or 97240 or fax to 503. Box 40384, portland, or 97204 or faxed to 503. Submit a written request and mail to: Medicare appeal and grievance unit p.o. Request for reconsideration should be sent to moda health, attn: Complaint and appeal form ready to submit? Mail this form to moda health, attn: Mail this form to moda health: Mail this form to moda health: Medicare appeals unit at p.o.

Fillable Online admissions cn revised appeal form 20072008.doc
Submit a written request and mail to: Mail this form to moda health: Mail this form to moda health: Request for reconsideration should be sent to moda health, attn: Mail this form to moda health, attn:

Online ODS COMPLAINT AND APPEAL Moda Doc Template pdfFiller
Complaint and appeal form ready to submit? Submit a written request and mail to: Box 40384, portland, or 97204 or faxed to 503. Medicare appeals unit at p.o. Medicare appeal and grievance unit p.o.

1st Appeal Format RTI 19 1 2005 PDF
Mail this form to moda health, attn: Mail this form to moda health: Complaint and appeal form ready to submit? Medicare appeal and grievance unit p.o. Submit a written request and mail to:

Dependency Override Appeal Form by SUNY Erie Issuu
Request for reconsideration should be sent to moda health, attn: Box 40384, portland, or 97204 or faxed to 503. Submit a written request and mail to: Mail this form to moda health: Mail this form to moda health, attn:
Erisa Appeal 20162024 Form Fill Out and Sign Printable PDF Template
Mail this form to moda health, attn: Submit a written request and mail to: Mail this form to moda health: Complaint and appeal form ready to submit? Request for reconsideration should be sent to moda health, attn:
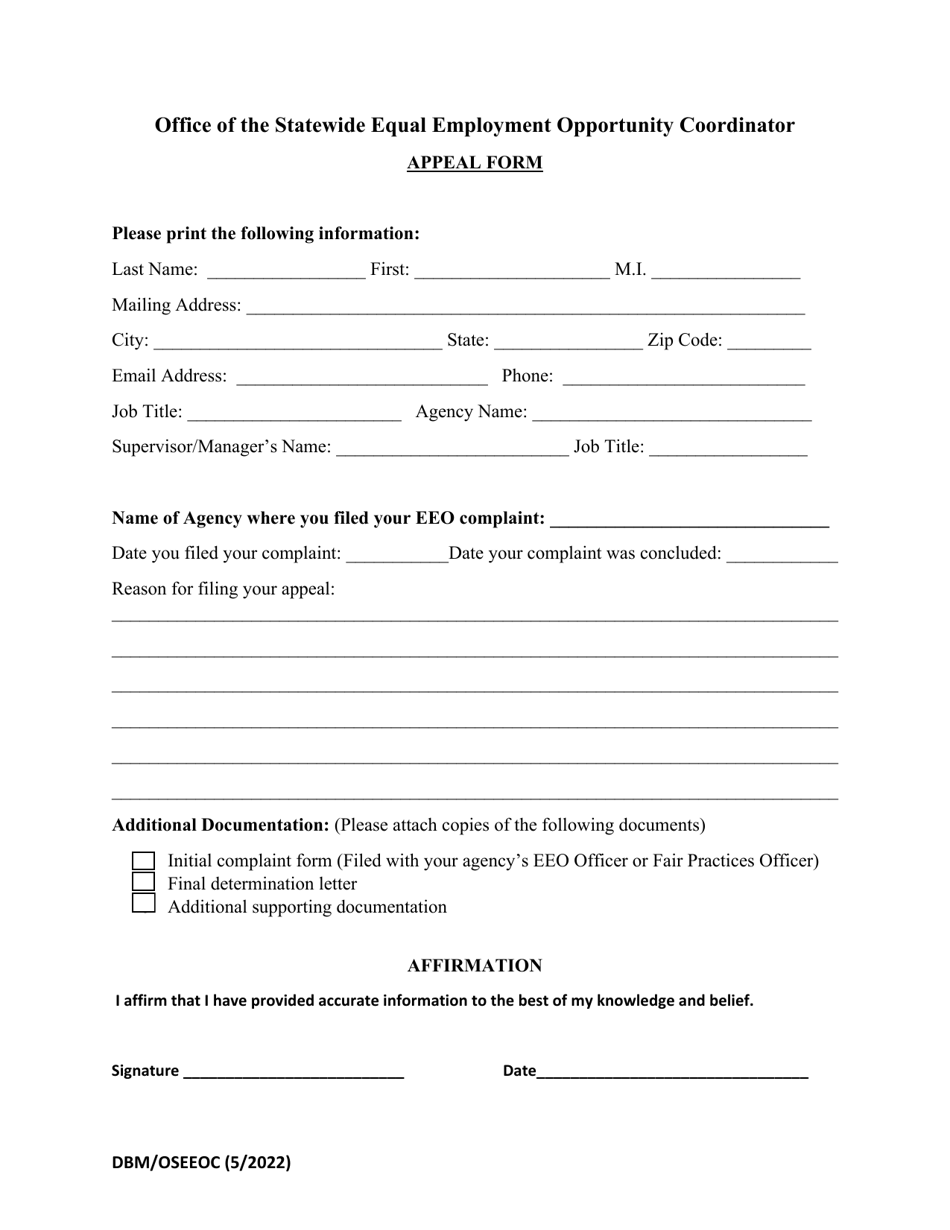
Maryland Office of the Statewide Equal Employment Opportunity
Mail this form to moda health: Submit a written request and mail to: Medicare appeals unit at p.o. Complaint and appeal form ready to submit? Mail this form to moda health, attn:
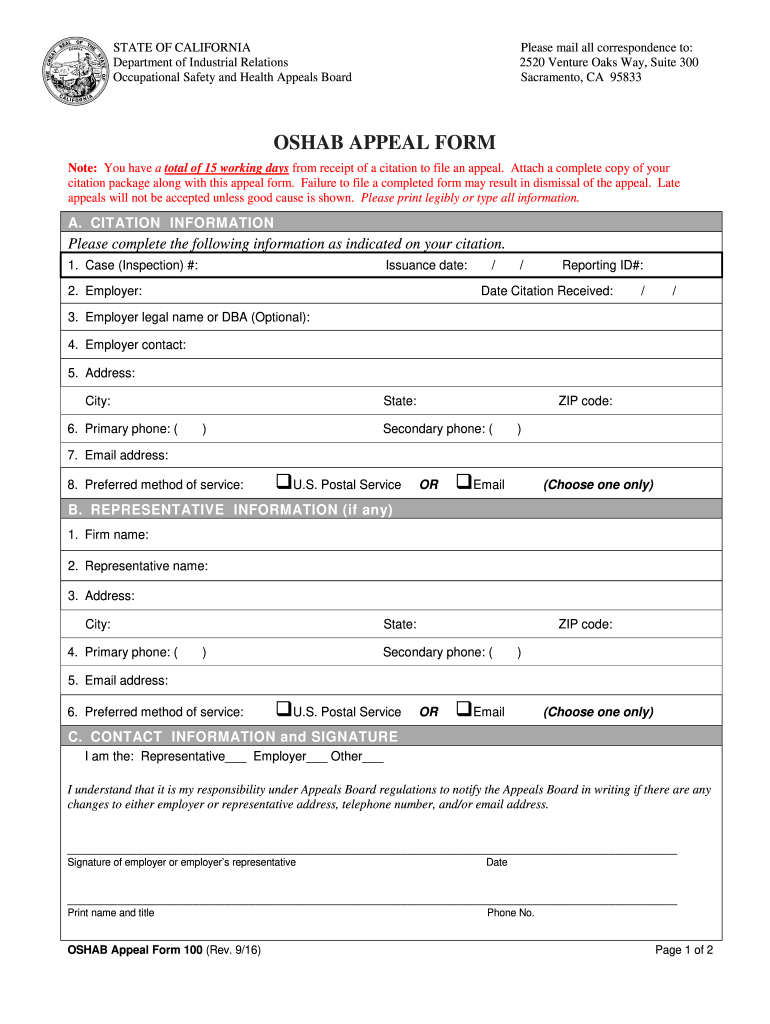
Ca Appeal Complete with ease airSlate SignNow
Submit a written request and mail to: Request for reconsideration should be sent to moda health, attn: Complaint and appeal form ready to submit? Mail this form to moda health: Medicare appeals unit at p.o.
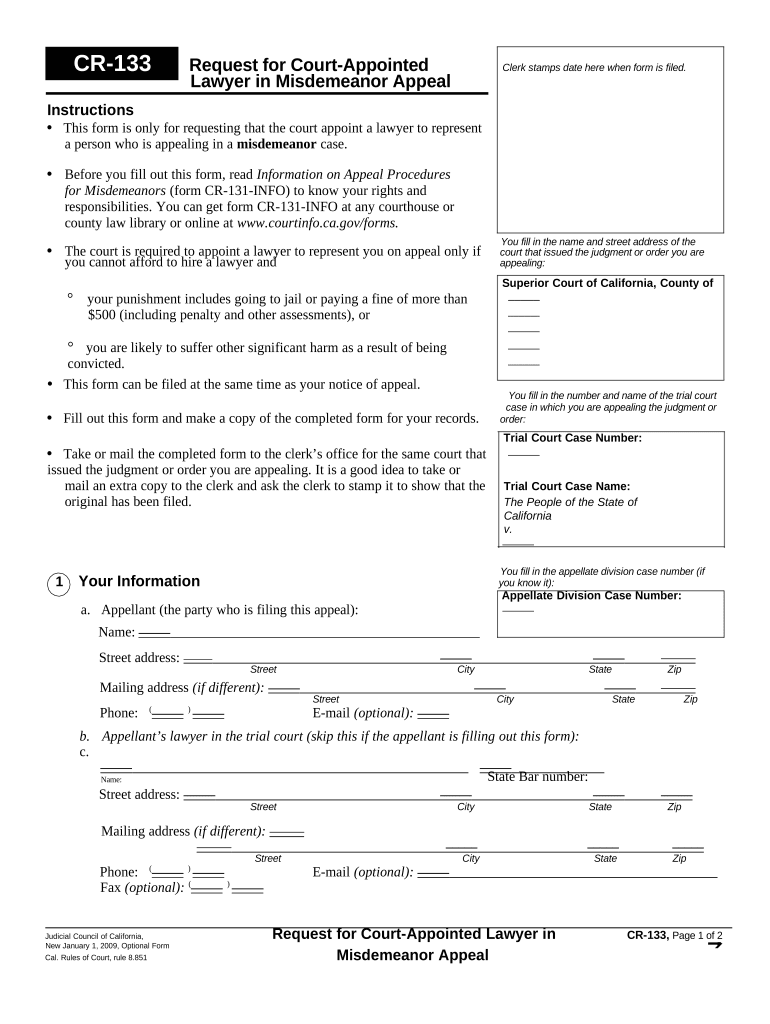
Misdemeanor Appeal Complete with ease airSlate SignNow
Complaint and appeal form ready to submit? Mail this form to moda health: Mail this form to moda health, attn: Medicare appeal and grievance unit p.o. Box 40384, portland, or 97204 or faxed to 503.

Fillable Online MAC Appeal Form Fax Email Print pdfFiller
Medicare appeals unit at p.o. Submit a written request and mail to: Complaint and appeal form ready to submit? Mail this form to moda health, attn: Medicare appeal and grievance unit p.o.

แจ้งเรื่องร้องเรียนการทุจริตและประพฤติมิชอบ โรงเรียนท่าเรือ "นิตยานุกูล"
Medicare appeal and grievance unit p.o. Medicare appeals unit at p.o. Mail this form to moda health: Request for reconsideration should be sent to moda health, attn: Mail this form to moda health:
Box 40384, Portland, Or 97204 Or Faxed To 503.
Request for reconsideration should be sent to moda health, attn: Mail this form to moda health: Medicare appeal and grievance unit p.o. Medicare appeals unit at p.o.
Complaint And Appeal Form Ready To Submit?
Mail this form to moda health, attn: Submit a written request and mail to: Box 40384, portland, or 97240 or fax to 503. Mail this form to moda health: