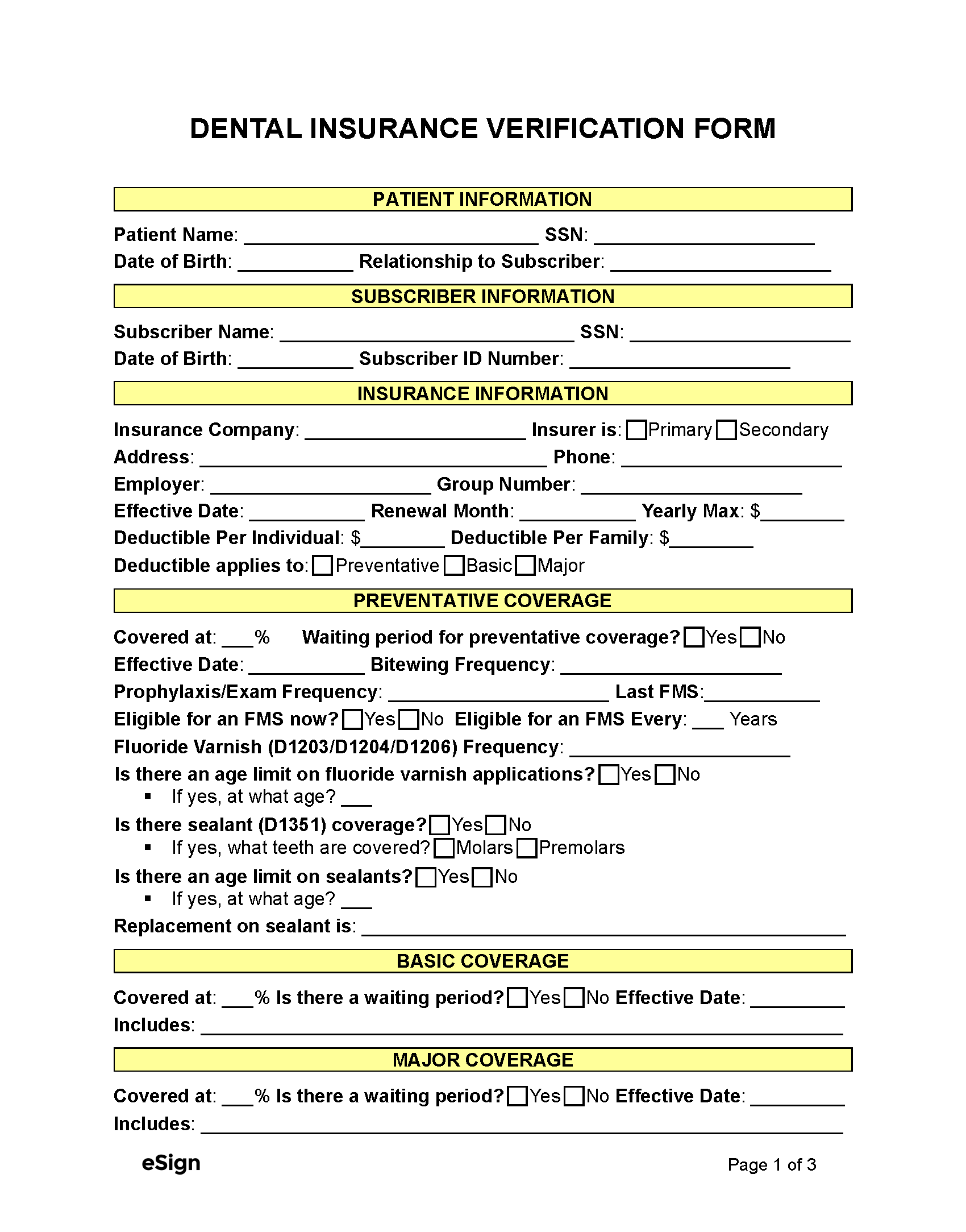
Insurance Breakdown Form
Insurance Breakdown Form - Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)?
Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)?

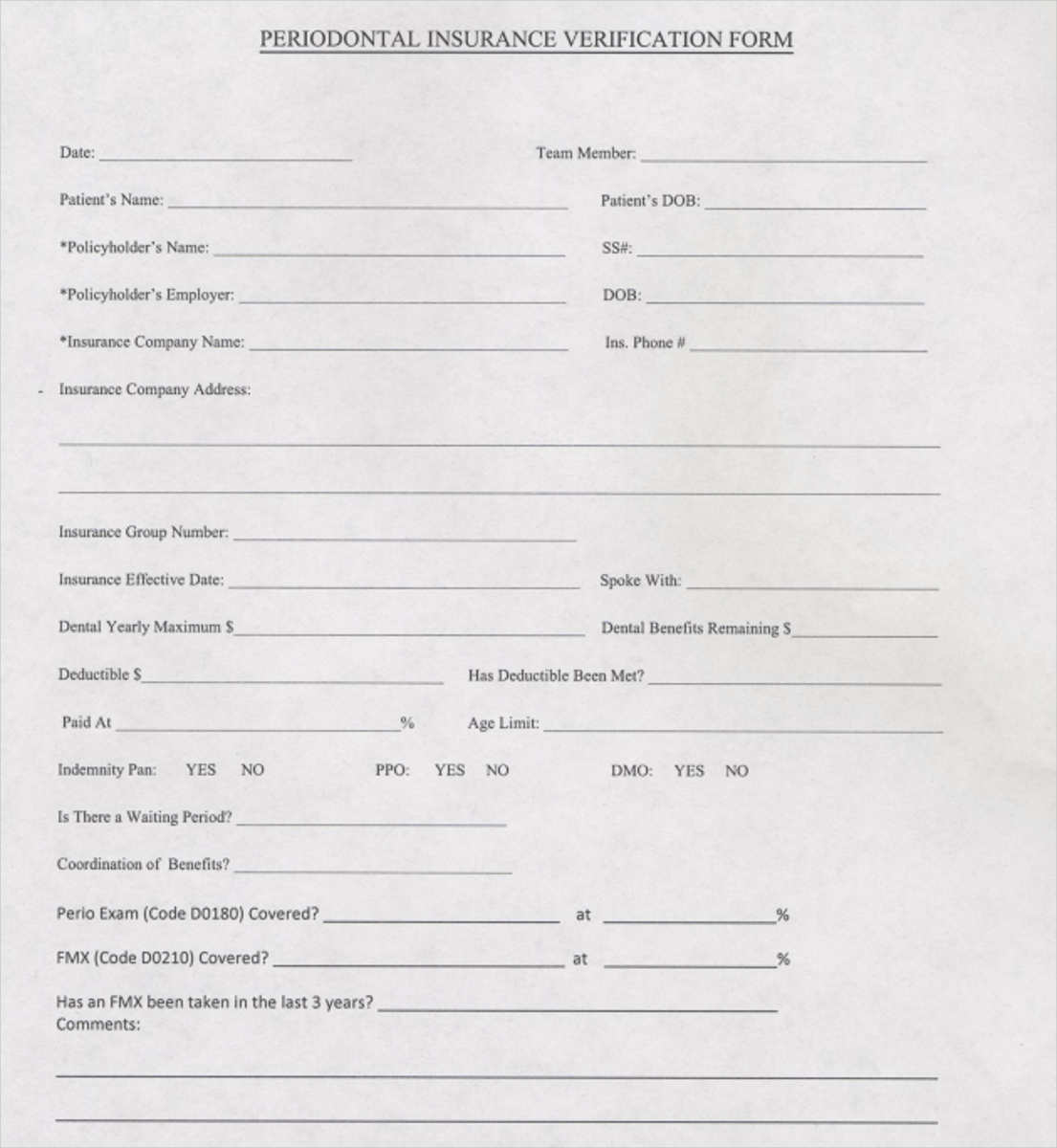
Template Dental Insurance Breakdown Form
Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)?
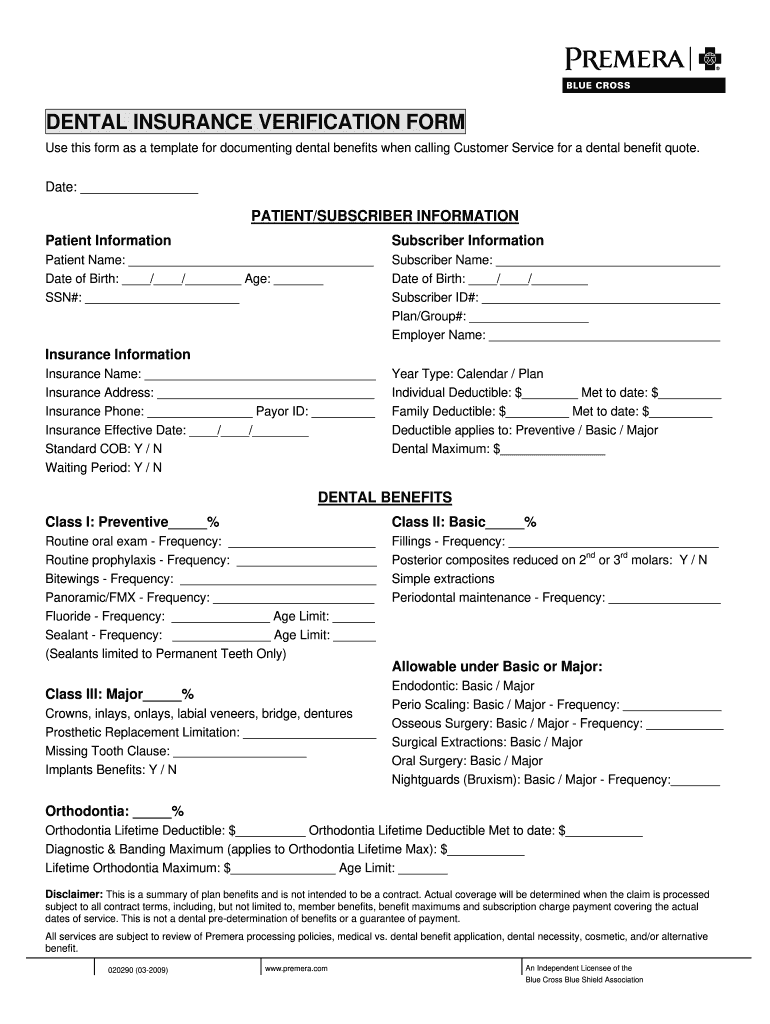
Free Dental Insurance Verification Form PDF Word
Insurance information does the patient have any history of srp (d4341/d4342)? Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____
best dental insurance
Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____

Dental Insurance Verification Form — The Superbill Blog
Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)?

Template Dental Insurance Breakdown Form INSURANCE DAY
Insurance information does the patient have any history of srp (d4341/d4342)? Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____
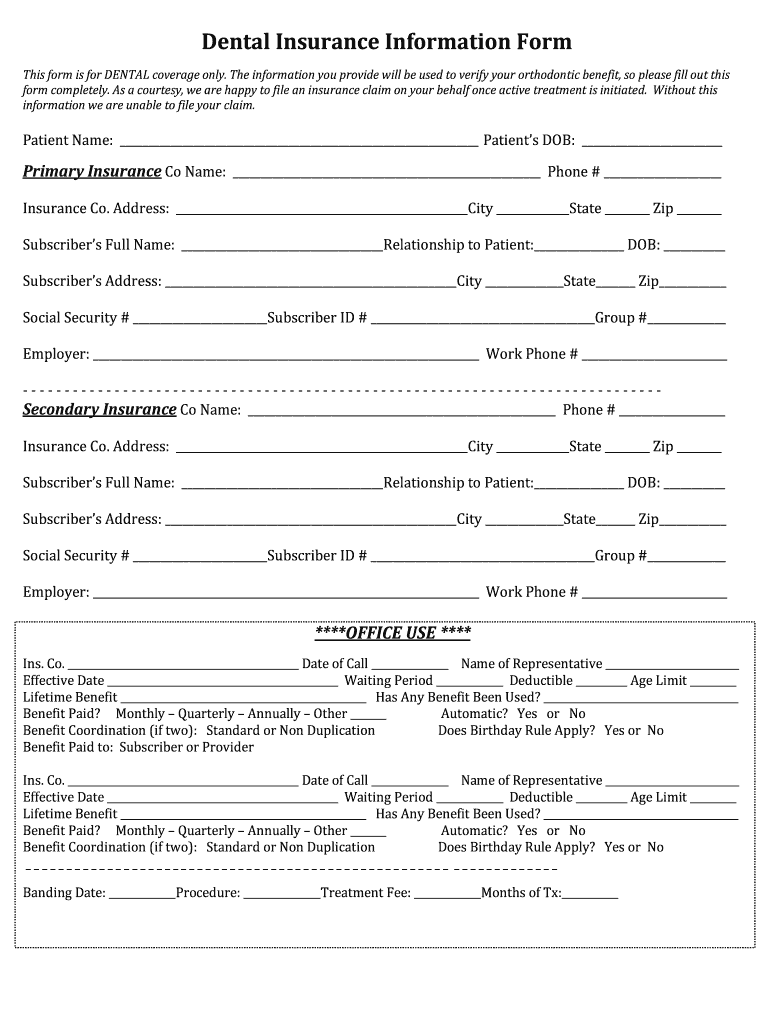
Dental Insurance Information Form Fill Online, Printable, Fillable
Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____

5 Tips Reviewing a Patient's Dental Insurance Breakdown Forms
Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?

Insurance Form Templates for Online Use 123 Form Builder
Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____
Dental Insurance Breakdown 20092024 Form Fill Out and Sign Printable
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)?

Template Dental Insurance Breakdown Form
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)?
Yes No If Yes, When?
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)?