Hipaa Release Form Michigan
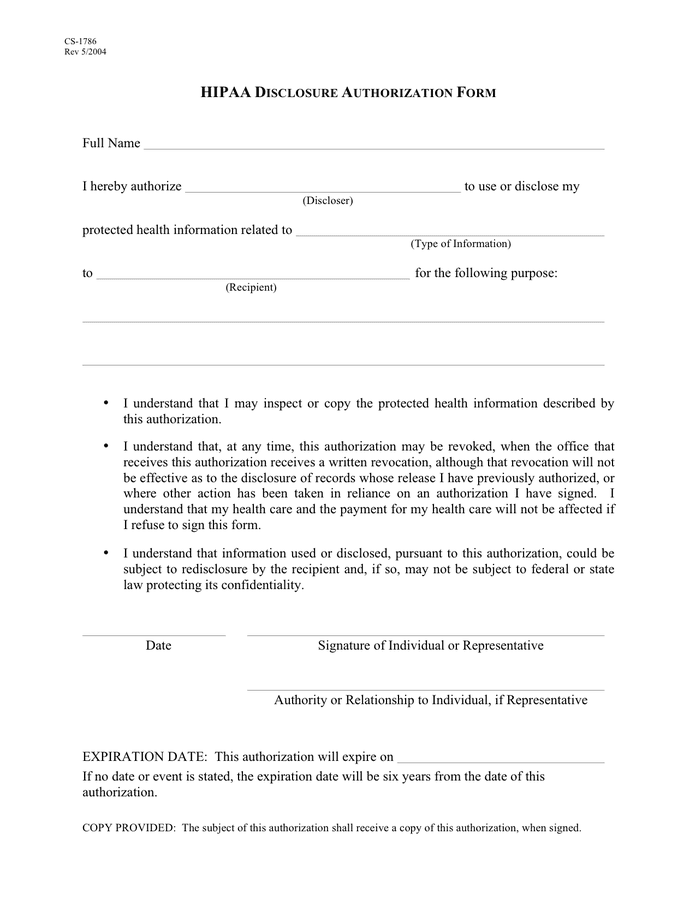
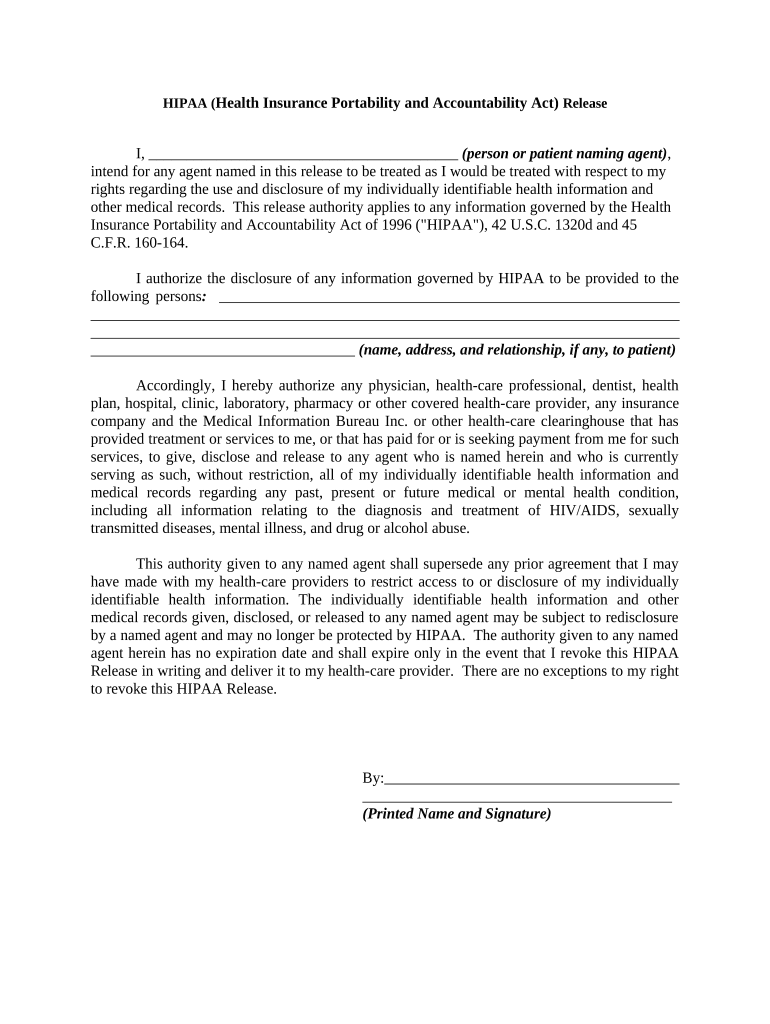
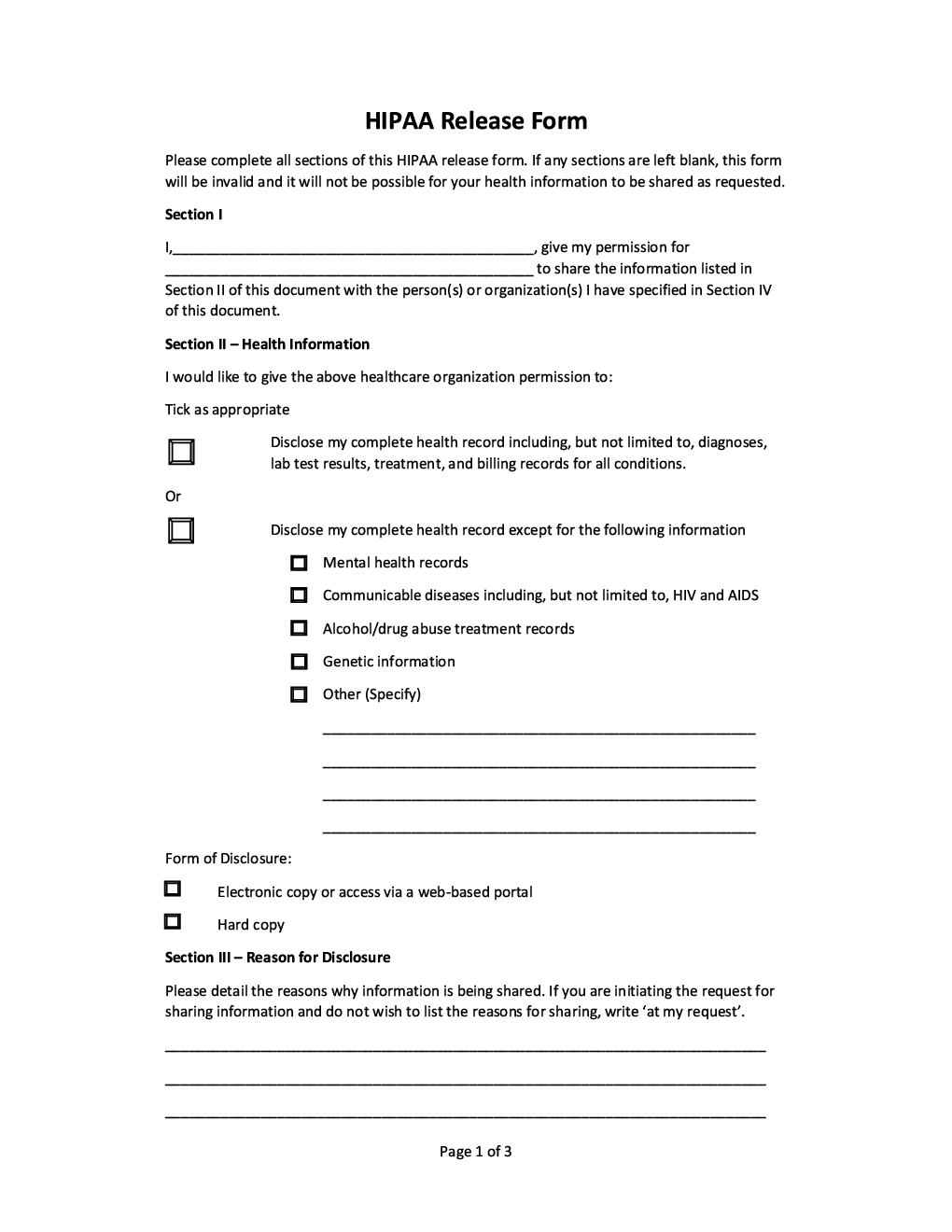
Hipaa Release Form Michigan - The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. Individuals that request the disclosure of their protected health information are urged to use the following authorization form that meets hipaa. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”), 42 usc.
Individuals that request the disclosure of their protected health information are urged to use the following authorization form that meets hipaa. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”), 42 usc. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information.
This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”), 42 usc. Individuals that request the disclosure of their protected health information are urged to use the following authorization form that meets hipaa.
HIPAA Disclosure Authorization Form Michigan in Word and Pdf formats
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Individuals that request the disclosure of their protected health information are urged to use the following authorization form that meets hipaa. Release authority applies to any information governed by the health insurance portability and accountability act.
HIPAA Form Printable Complete with ease airSlate SignNow
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”),.
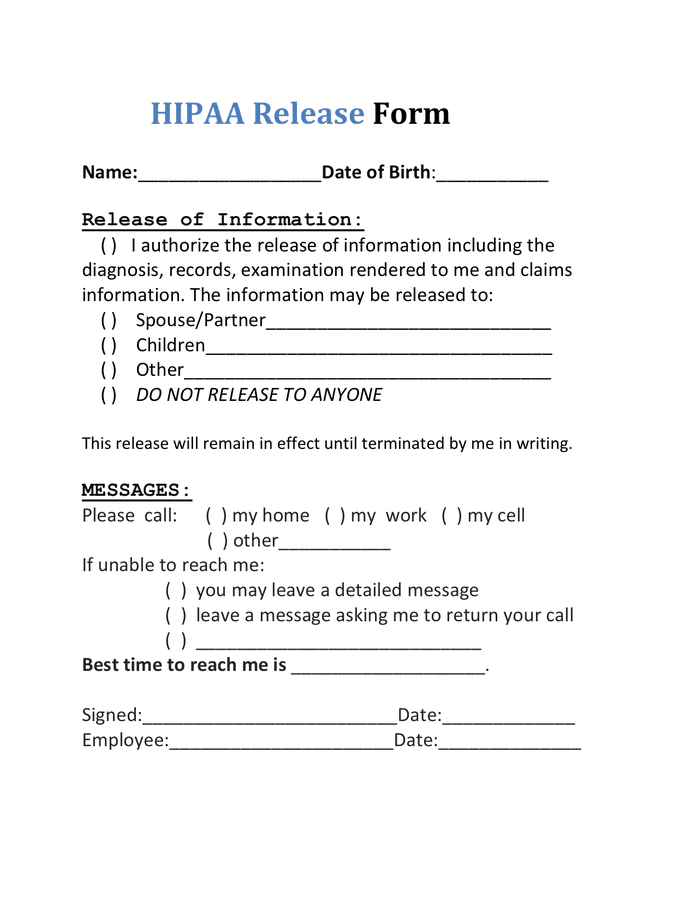
Printable Hipaa Release Form
Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”),.
Printable Hipaa Release Form Pennsylvania Printable Forms Free Online
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”), 42 usc. This form is acceptable to the michigan department of health and human services as compliant with.
HIPAA release form Forms Docs 2023
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. Individuals that request the disclosure of their protected health information are urged to use the following authorization form.
Legal Utah Courts Hipaa Information Release Form Printable Printable
This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. Individuals that request the disclosure of their protected health information are urged to use the following authorization form that meets hipaa. Release authority applies.
FREE 9+ Sample Hipaa Forms in PDF MS Word
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”),.
Fillable Hipaa Release Form California Printable Forms Free Online
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information..

HIPAA Release Form What is a HIPAA Authorization Form?
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy..
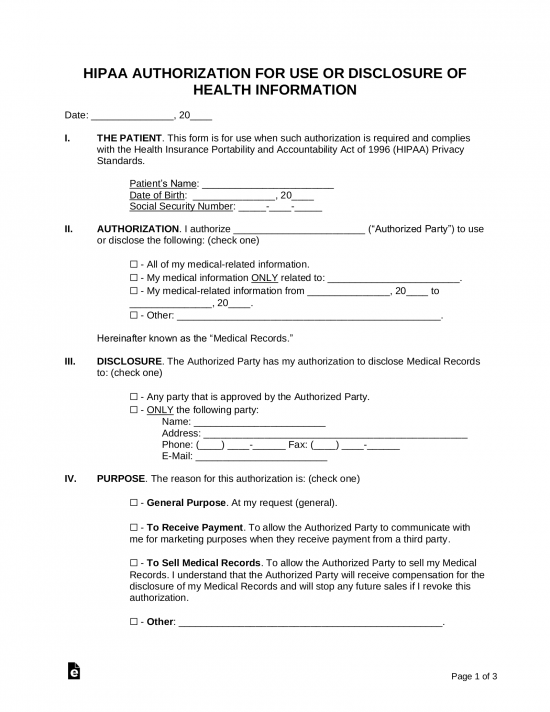
Free HIPAA Medical Release Authorization Form PDF
The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information..
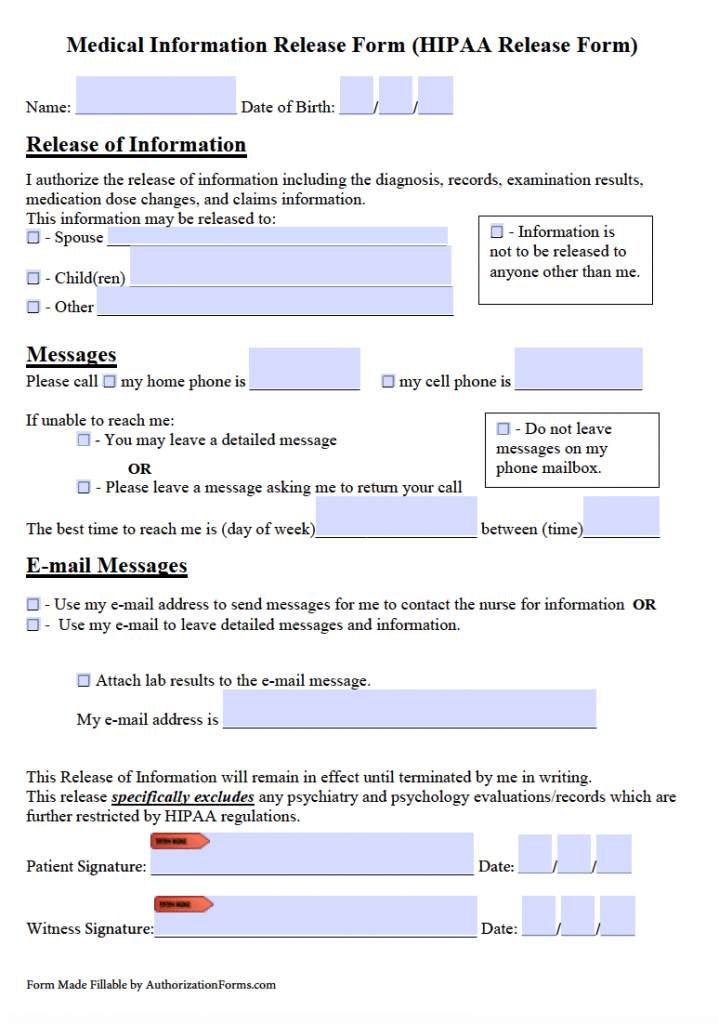
Individuals That Request The Disclosure Of Their Protected Health Information Are Urged To Use The Following Authorization Form That Meets Hipaa.
Release authority applies to any information governed by the health insurance portability and accountability act of 1996 (“hipaa”), 42 usc. Hipaa disclosure authorization form full name i hereby authorize (discloser) to use or disclose my protected health information. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy. The custodian will deliver to the requesting party the original information or a true and exact copy of the original information accompanied by the.