Hhccn Form Home Health
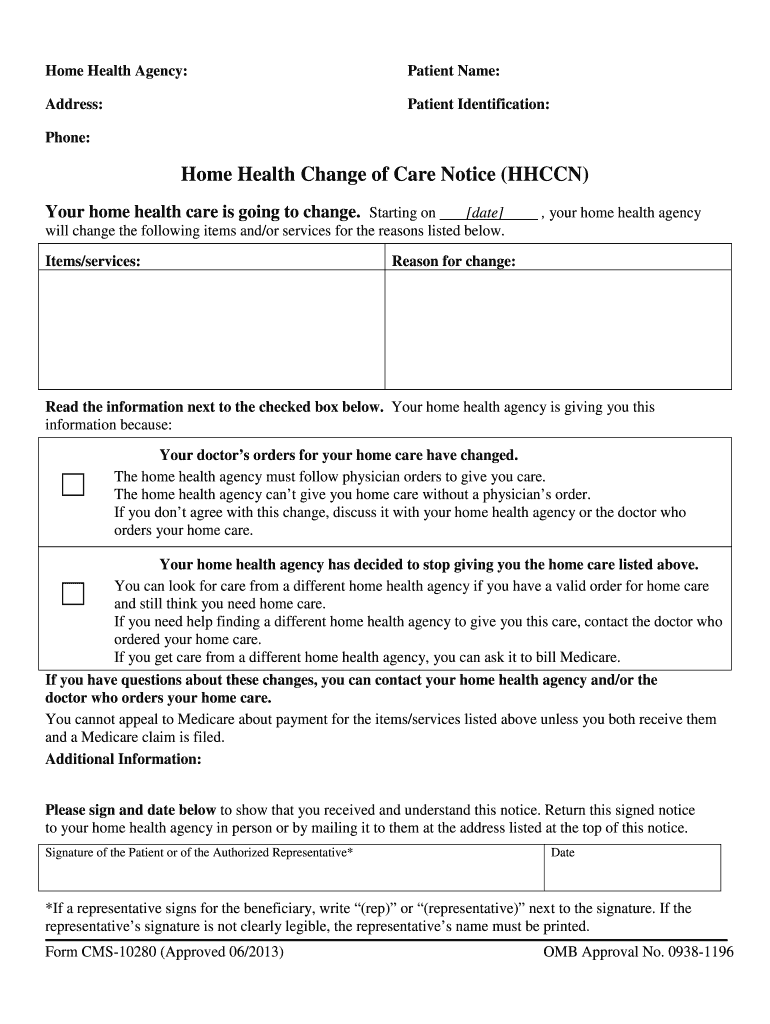
Hhccn Form Home Health - Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the.
This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior.
This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original.

Instructions for the HHCCN CMS Doc Template pdfFiller
Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior..

Home Health Change of Care Notice (HHCCN) Spanish DIGITAL FORM
Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Request for.
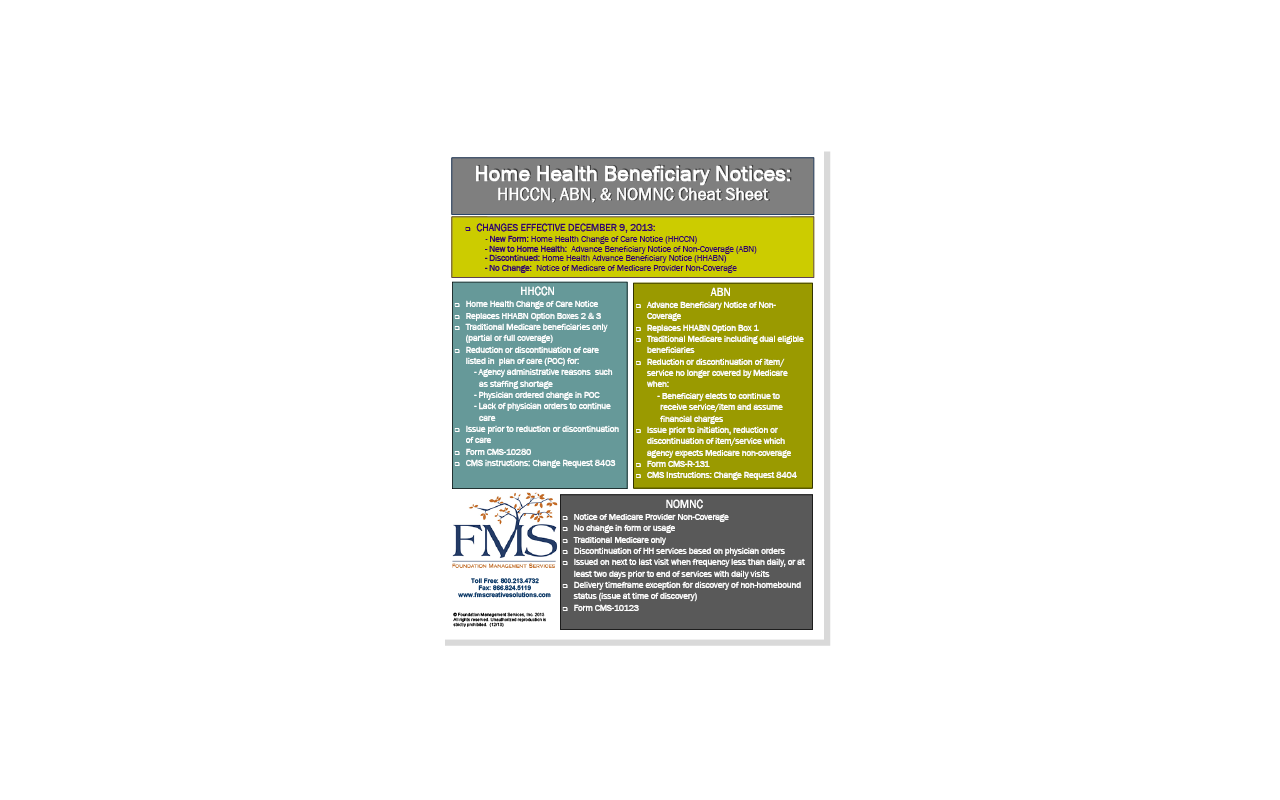
FMS is MAC Legacy Home Health Beneficary Notices HHCCN, ABN
Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the..

Fillable Online Home Health Change Of Care Notice Hhccn Form. Home
This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior..

Fillable Online HHCCN Form Instructions (PDF) Fax Email Print pdfFiller
Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. This information collection is for.

NEW HHCCN Form for Home Health Agencies National Association for Home
Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. This information collection is for.
Hhccn 20132024 Form Fill Out and Sign Printable PDF Template
This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. Hhccn whenever.

Home Health Change of Care Notice (HHCCN) DIGITAL FORM
Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Request for.
Renewal of the HHCCN PMB
This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. Hhccn whenever.

Completing the NOMNC, ABN and HHCCN forms YouTube
This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Request for hcpcs code addition medicaid home health fee schedule (dma3400) the following form can be found nctracks prior. Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. Hhccn whenever.
Request For Hcpcs Code Addition Medicaid Home Health Fee Schedule (Dma3400) The Following Form Can Be Found Nctracks Prior.
Home health agencies (hhas) are responsible for issuing the following beneficiary rights and protections notices to original. This information collection is for the home health agencies to notify original medicare beneficiaries receiving home health care benefits of plan of. Hhccn whenever they reduce or terminate a beneficiary’s home health services due to physician/provider orders or limitations of the.