Designation Of Authorized Representative Form
Designation Of Authorized Representative Form - This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. _________________________________________________________ to act as my authorized representative. The form has two sections: Download and print this form to designate a person or entity to act on your behalf with medicaid. This individual is an adult who is sufficiently aware of.
Download and print this form to designate a person or entity to act on your behalf with medicaid. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. _________________________________________________________ to act as my authorized representative. This individual is an adult who is sufficiently aware of. The form has two sections:
The form has two sections: _________________________________________________________ to act as my authorized representative. Download and print this form to designate a person or entity to act on your behalf with medicaid. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. This individual is an adult who is sufficiently aware of. This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an.

Authorized Representative Designation Form PDF Professional Ethics
This individual is an adult who is sufficiently aware of. Download and print this form to designate a person or entity to act on your behalf with medicaid. This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. _________________________________________________________ to act as my authorized representative. Download and fill.
Fillable Online Authorized Representative Designation Form Mass.gov
_________________________________________________________ to act as my authorized representative. Download and print this form to designate a person or entity to act on your behalf with medicaid. The form has two sections: This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. Download and fill out this form to designate.
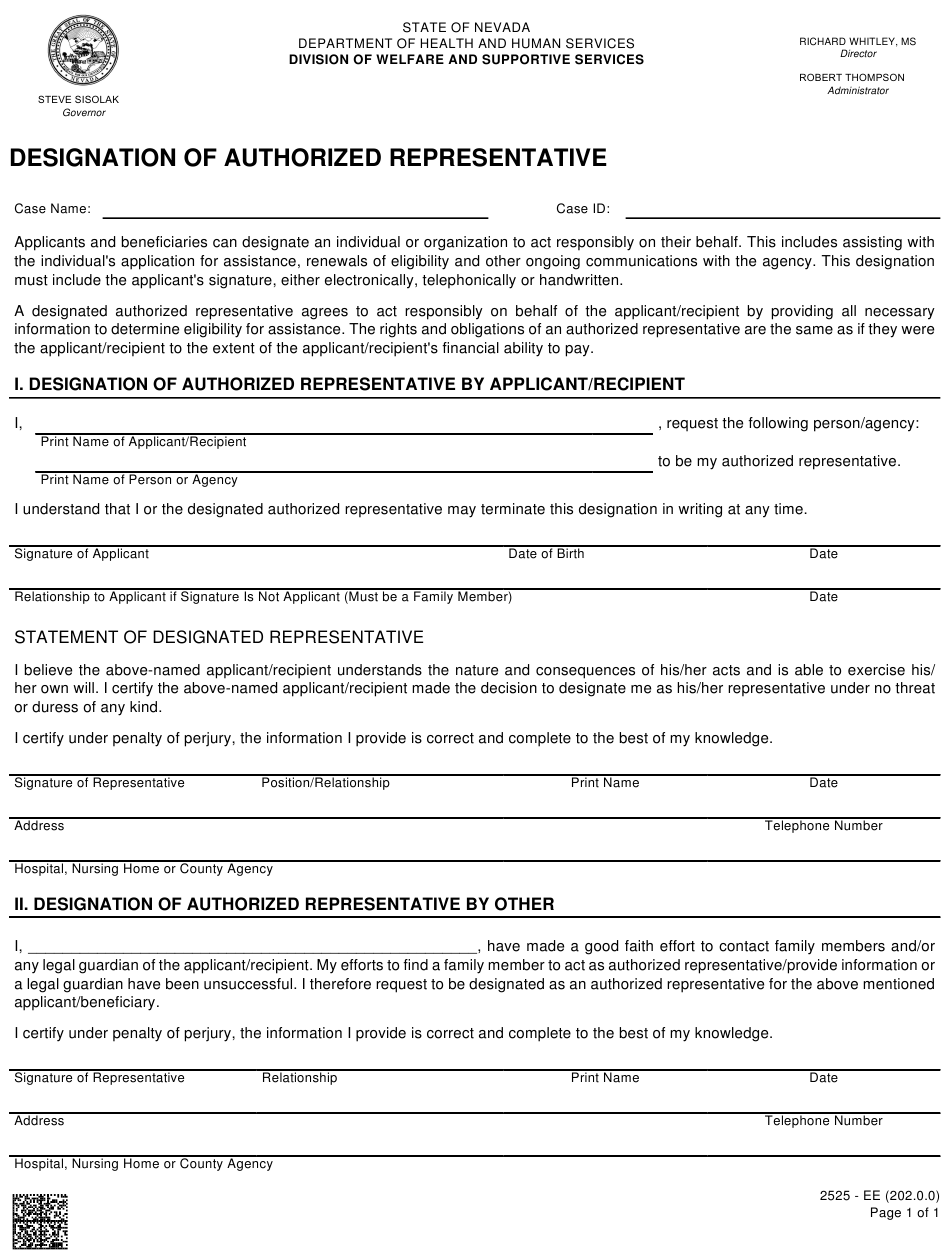
Form 2525EE Download Fillable PDF or Fill Online Designation of
Download and print this form to designate a person or entity to act on your behalf with medicaid. The form has two sections: This individual is an adult who is sufficiently aware of. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. _________________________________________________________ to act as my.

Uhc Designation Of Authorized Representative Form
Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. Download and print this form to designate a person or entity to act on your behalf with medicaid. This individual is an adult who is sufficiently aware of. This form is for releasing health information to another person.
Sample Designation Of Authorized Representative Form printable pdf download
The form has two sections: This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. Download and print this form to designate a person or entity to act on your behalf with medicaid. Download and fill out this form to designate an authorized representative to act on your.
Member authorization form for a designated representative in Word and
The form has two sections: Download and print this form to designate a person or entity to act on your behalf with medicaid. This individual is an adult who is sufficiently aware of. _________________________________________________________ to act as my authorized representative. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health.
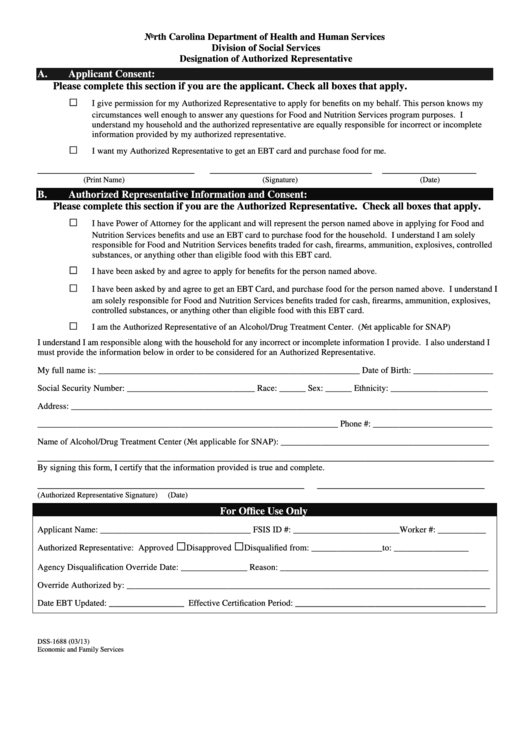
Fillable Form Dss1688 Designation Of Authorized Representative
The form has two sections: This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. Download and print this form to designate a person or entity to act on your behalf with medicaid. This individual is an adult who is sufficiently aware of. Download and fill out this.
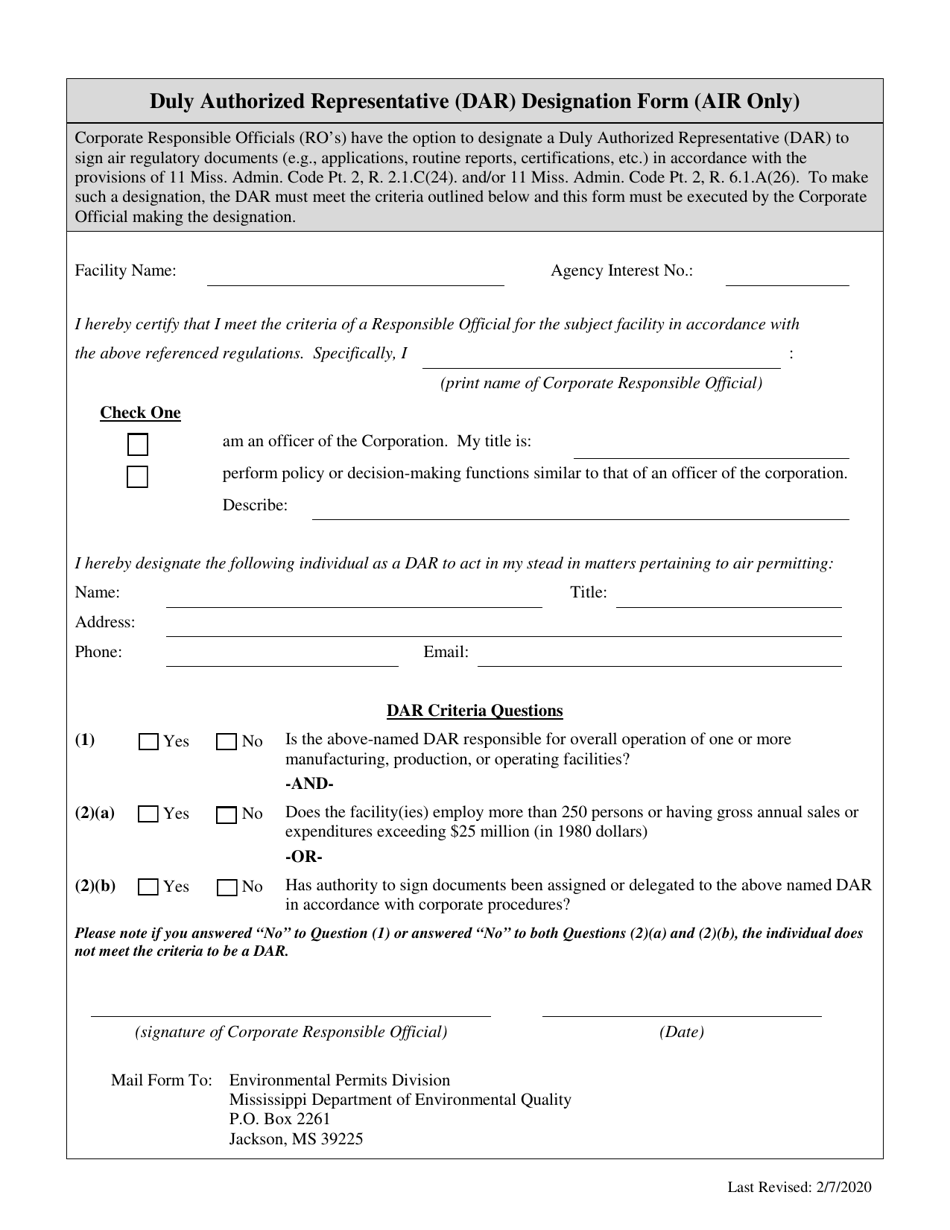
Mississippi Duly Authorized Representative (Dar) Designation Form (Air
Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. The form has two sections: This individual is an adult who is sufficiently aware of. _________________________________________________________ to act as my authorized representative. This form is for releasing health information to another person or company or appointing an authorized.
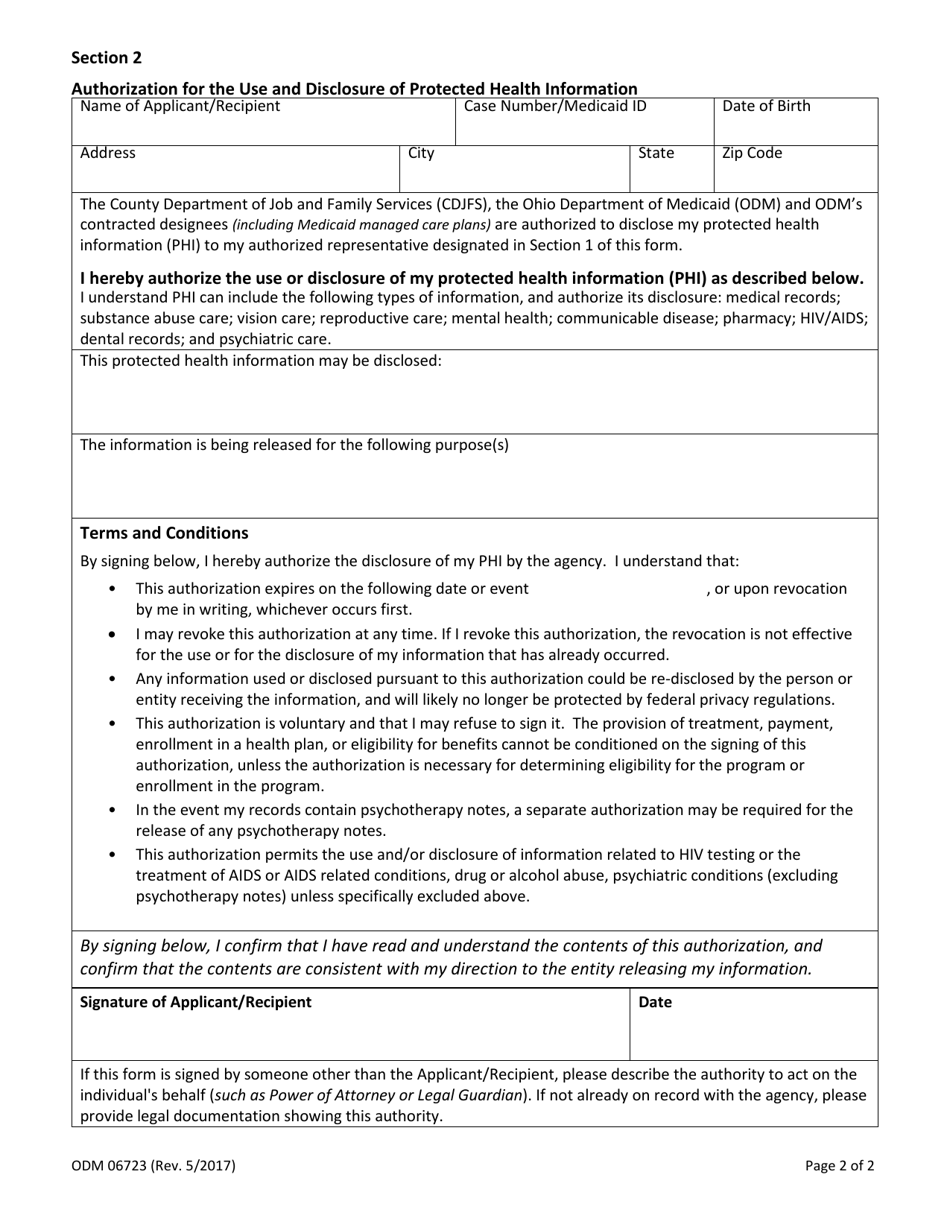
Form ODM06723 Fill Out, Sign Online and Download Fillable PDF, Ohio
Download and print this form to designate a person or entity to act on your behalf with medicaid. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. This individual is an adult who is sufficiently aware of. _________________________________________________________ to act as my authorized representative. This form is.
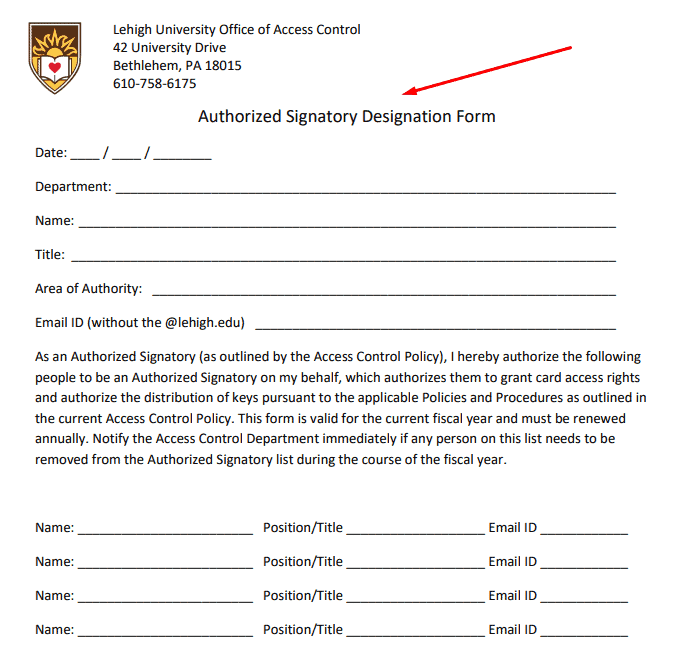
What Is An Authorized Signatory (Legal Definition And Examples)
The form has two sections: This individual is an adult who is sufficiently aware of. Download and print this form to designate a person or entity to act on your behalf with medicaid. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs. This form is for releasing.
_________________________________________________________ To Act As My Authorized Representative.
This individual is an adult who is sufficiently aware of. Download and print this form to designate a person or entity to act on your behalf with medicaid. This form is for releasing health information to another person or company or appointing an authorized representative for a grievance or an. Download and fill out this form to designate an authorized representative to act on your behalf for masshealth and health connector programs.