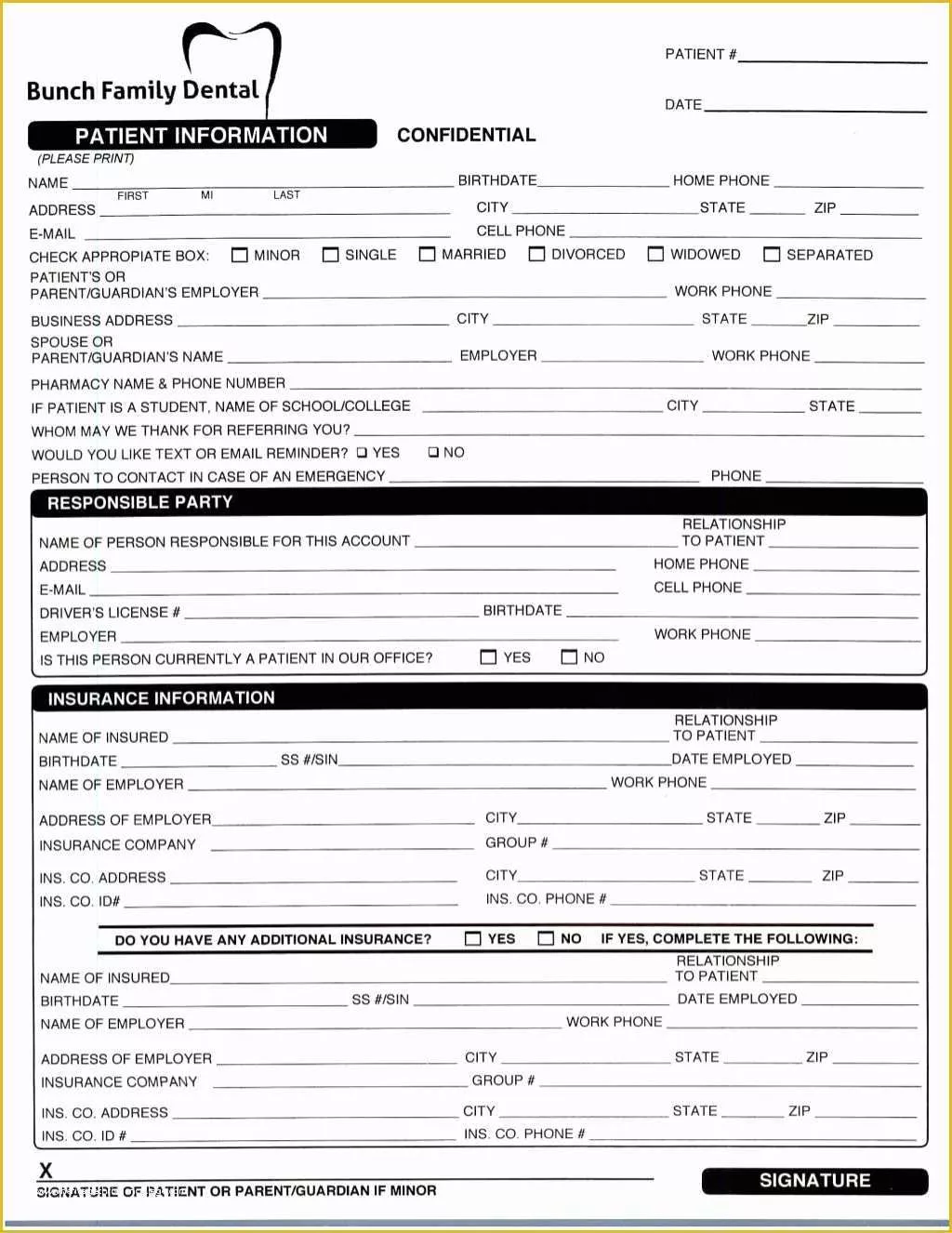
Dental Patient Registration Form Pdf
Dental Patient Registration Form Pdf - Asking you about your health or dental care plans, or other sources of payment; Do you want to learn to control your dental disease and retain your teeth ? Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Please read this form carefully and ask. I certify that i have read and. As a condition of treatment by this office, i understand financial. Any disease, condition or problem not listed ? State law requires our office to obtain your consent for your contemplated oral care and dental treatment. The financial responsibility of each patient must be determined before treatment.
I certify that i have read and. Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment. Any disease, condition or problem not listed ? Asking you about your health or dental care plans, or other sources of payment; Do you want to learn to control your dental disease and retain your teeth ? Information for payment purposes are: The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. The financial responsibility of each patient must be determined before treatment. Please read this form carefully and ask. As a condition of treatment by this office, i understand financial.
I certify that i have read and. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Information for payment purposes are: The financial responsibility of each patient must be determined before treatment. State law requires our office to obtain your consent for your contemplated oral care and dental treatment. Asking you about your health or dental care plans, or other sources of payment; As a condition of treatment by this office, i understand financial. Any disease, condition or problem not listed ? Do you want to learn to control your dental disease and retain your teeth ? Please read this form carefully and ask.
Printable Dental Patient Registration Form Template
The financial responsibility of each patient must be determined before treatment. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment. State law requires our office to obtain your consent.

Free printable dental forms Fill out & sign online DocHub
I certify that i have read and. State law requires our office to obtain your consent for your contemplated oral care and dental treatment. Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment. As a condition of treatment by this office, i understand financial. The financial responsibility of each patient must.

Dental Patient Registration form Template Inspirational 27 Of Dental
Information for payment purposes are: Please read this form carefully and ask. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. I certify that i have read and. The financial responsibility of each patient must be determined before treatment.
FREE 9+ Patient Registration Form Samples in PDF Excel MS Word
State law requires our office to obtain your consent for your contemplated oral care and dental treatment. Information for payment purposes are: As a condition of treatment by this office, i understand financial. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. I certify that i have.
FREE 9+ Patient Registration Form Samples in PDF Excel MS Word
State law requires our office to obtain your consent for your contemplated oral care and dental treatment. Asking you about your health or dental care plans, or other sources of payment; Do you want to learn to control your dental disease and retain your teeth ? Please read this form carefully and ask. I certify that i have read and.
Forms Idaho Falls Dentist Legacy Dental
Please read this form carefully and ask. I certify that i have read and. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Any disease, condition or problem not listed ? Information for payment purposes are:
Downloadable dental forms Patient registration form Dentistry IQ
Do you want to learn to control your dental disease and retain your teeth ? Please read this form carefully and ask. Asking you about your health or dental care plans, or other sources of payment; The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. I certify.
Printable Dental Patient Registration Form Template
Please read this form carefully and ask. Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment. As a condition of treatment by this office, i understand financial. State law requires our office to obtain your consent for your contemplated oral care and dental treatment. Information for payment purposes are:

printable dental patient registration form template sample in 2021
Please read this form carefully and ask. Any disease, condition or problem not listed ? Do you want to learn to control your dental disease and retain your teeth ? I certify that i have read and. The financial responsibility of each patient must be determined before treatment.

28 Dental Patient Registration form Template in 2020 Registration
Do you want to learn to control your dental disease and retain your teeth ? Any disease, condition or problem not listed ? Please read this form carefully and ask. The financial responsibility of each patient must be determined before treatment. Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment.
State Law Requires Our Office To Obtain Your Consent For Your Contemplated Oral Care And Dental Treatment.
Please read this form carefully and ask. As a condition of treatment by this office, i understand financial. Do you want to learn to control your dental disease and retain your teeth ? Asking you about your health or dental care plans, or other sources of payment;
I Certify That I Have Read And.
Any disease, condition or problem not listed ? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Both doctor and patient are encouraged to discuss any and all relevent patient health issues prior to treatment. Information for payment purposes are: