Car Accident Intake Form
Car Accident Intake Form - Were you taken to the hospital after the accident? If your vehicle was moving at the time of impact, was it: _____ describe your condition and symptoms caused by the accident:. Information pertaining to you and the car you were in year: When and where did the. _____ year and make of other driver(s) vehicle: Have you ever been involved in a motor vehicle accident before? Did you lose consciousness during the accident? Make & model of other vehicle: Describe how the accident took place:
_____ describe your condition and symptoms caused by the accident:. When and where did the. Did you lose consciousness during the accident? Have you ever been involved in a motor vehicle accident before? _____ year and make of other driver(s) vehicle: Year and make of client’s vehicle: How fast was the other vehicle going? Make & model of other vehicle: Slowing down gaining speed steady speed other. If yes, please answer the five questions below:
Did you lose consciousness during the accident? Year and make of client’s vehicle: Were you taken to the hospital after the accident? Make & model of other vehicle: Which direction was the other vehicle heading? Has your primary care doctor or any other. Describe how the accident took place: _____ describe your condition and symptoms caused by the accident:. Have you ever been involved in a motor vehicle accident before? _____ passenger and/or witnesses’ information:

Personal injury forms Fill out & sign online DocHub
If yes, please answer the five questions below: Which direction was the other vehicle heading? Information pertaining to you and the car you were in year: Did you lose consciousness during the accident? Has your primary care doctor or any other.

Downloadable Car Accident Information Form
_____ year and make of other driver(s) vehicle: When and where did the. If your vehicle was moving at the time of impact, was it: How fast was the other vehicle going? Have you ever been involved in a motor vehicle accident before?

Traffic Accident form Best Of Minnesota Motor Vehicle Crash Report
Were you taken to the hospital after the accident? Year and make of client’s vehicle: Slowing down gaining speed steady speed other. Information pertaining to you and the car you were in year: How fast was the other vehicle going?

Chiropractic new patient intake form Fill out & sign online DocHub
Slowing down gaining speed steady speed other. _____ passenger and/or witnesses’ information: Describe how the accident took place: Make & model of other vehicle: Information pertaining to you and the car you were in year:

Car Accident Intake Form Lark Chiropractic
Year and make of client’s vehicle: If your vehicle was moving at the time of impact, was it: Did you lose consciousness during the accident? _____ passenger and/or witnesses’ information: Describe how the accident took place:

Fillable Online Motor Vehicle Accident New Patient Intake Forms Fax
Slowing down gaining speed steady speed other. _____ passenger and/or witnesses’ information: Did you lose consciousness during the accident? Have you ever been involved in a motor vehicle accident before? Were you taken to the hospital after the accident?
Fillable Online Personal Injury Intake Form (NonAuto Fax Email Print
Make & model of other vehicle: Have you ever been involved in a motor vehicle accident before? Has your primary care doctor or any other. _____ year and make of other driver(s) vehicle: Which direction was the other vehicle heading?
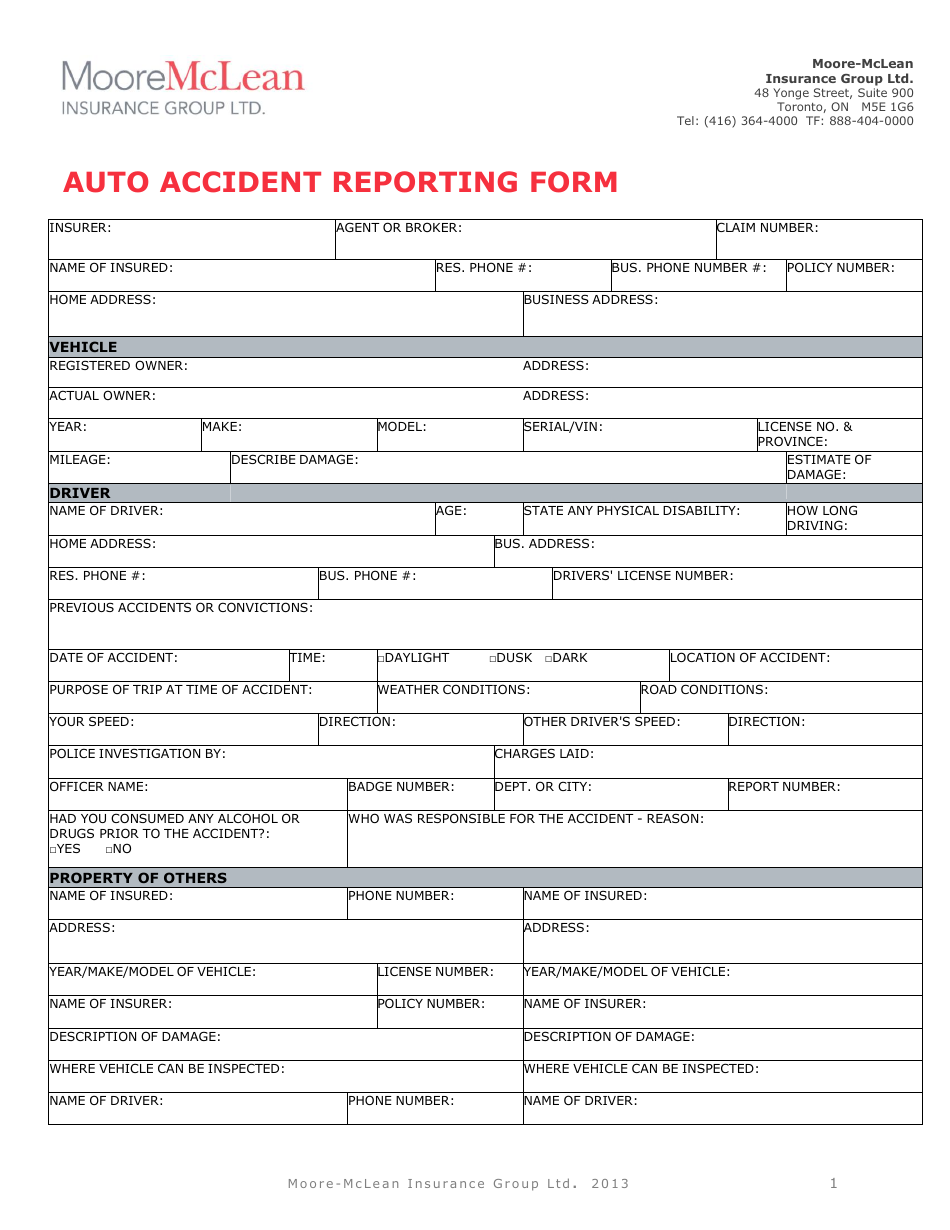
Auto Accident Reporting Form Mclean Hallmark Insurance Group Ltd
_____ passenger and/or witnesses’ information: Did you lose consciousness during the accident? _____ describe your condition and symptoms caused by the accident:. If yes, please answer the five questions below: Were you taken to the hospital after the accident?
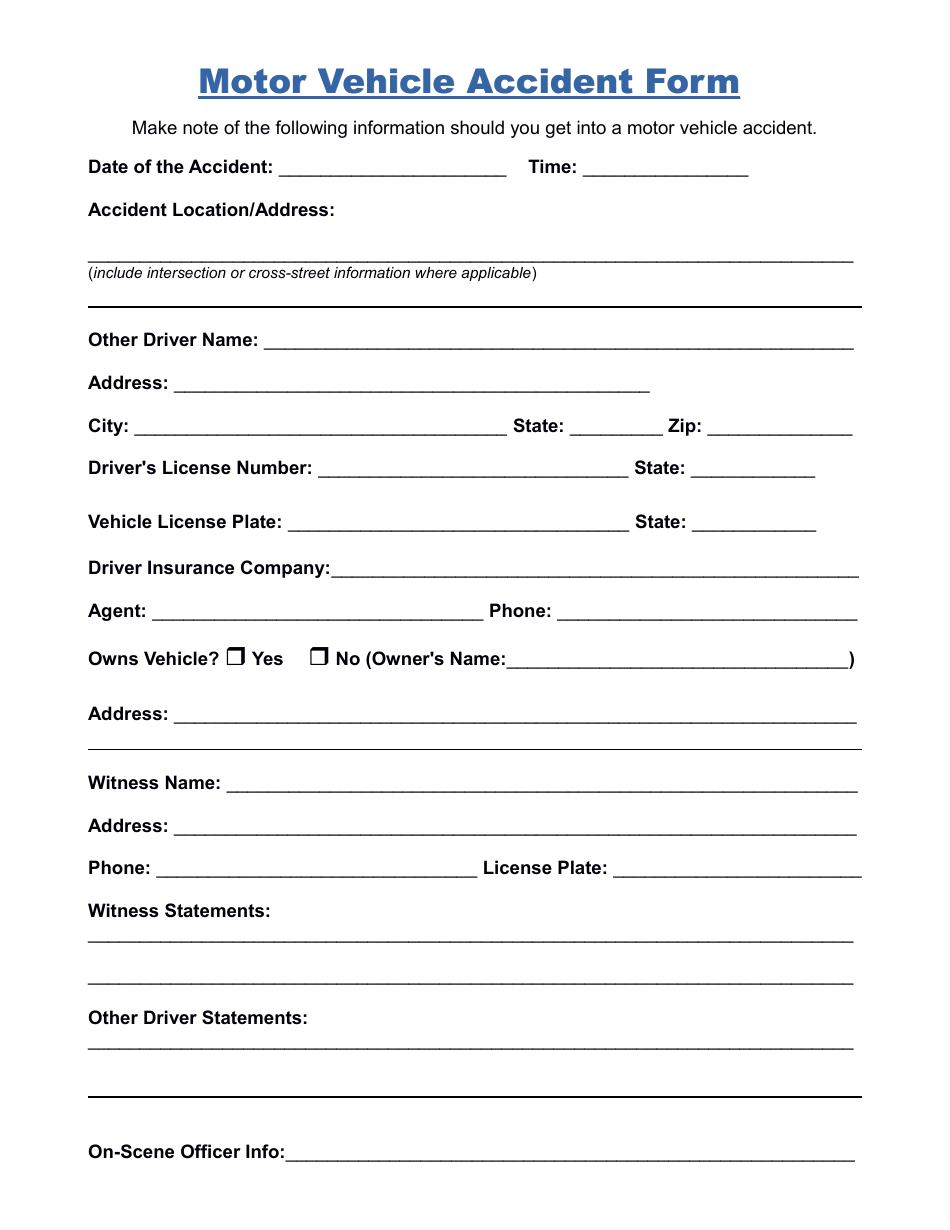
Motor Vehicle Accident Form Fill Out, Sign Online and Download PDF
_____ passenger and/or witnesses’ information: Slowing down gaining speed steady speed other. Have you ever been involved in a motor vehicle accident before? Year and make of client’s vehicle: Describe how the accident took place:
Intake Sheet Complete with ease airSlate SignNow
Describe how the accident took place: Have you ever been involved in a motor vehicle accident before? Has your primary care doctor or any other. _____ year and make of other driver(s) vehicle: _____ passenger and/or witnesses’ information:
Were You Taken To The Hospital After The Accident?
Has your primary care doctor or any other. _____ describe your condition and symptoms caused by the accident:. When and where did the. Information pertaining to you and the car you were in year:
_____ Year And Make Of Other Driver(S) Vehicle:
Did you lose consciousness during the accident? Have you ever been involved in a motor vehicle accident before? How fast was the other vehicle going? Make & model of other vehicle:
If Yes, Please Answer The Five Questions Below:
Describe how the accident took place: Which direction was the other vehicle heading? _____ passenger and/or witnesses’ information: Slowing down gaining speed steady speed other.
If Your Vehicle Was Moving At The Time Of Impact, Was It:
Year and make of client’s vehicle: